
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
💓Atrial flutter ✅
Related Subjects: |Wolff-Parkinson White syndrome (WPW) AVRT |Lown Ganong Levine Syndrome AVRT |Supraventricular Tachycardia (SVT) |Atrioventricular Nodal Reentrant Tachycardia AVNRT |Atrial Flutter |Atrial Fibrillation |Sinus Tachycardia |Sinus Arrhythmia |Multifocal Atrial Tachycardia |Resuscitation - Adult Tachycardia Algorithm |AF and Anticoagulation
⚠️ Important: Class I antiarrhythmics (e.g. flecainide) must be used with AV nodal blockade (β-blocker or rate-limiting calcium channel blocker) to prevent dangerous 1:1 AV conduction ⚡. ❌ Avoid antiarrhythmic monotherapy in atrial flutter. 🔥 Catheter ablation (targeting the re-entrant circuit) has >90% success and is first-line definitive therapy in typical flutter.
ℹ️ About Atrial Flutter
- ⚡ Atrial rate: 280–350 bpm due to a macro-reentrant circuit.
- 🧐 Ventricular rate typically ~150 bpm with 2:1 AV block.
- 🔄 Often alternates with atrial fibrillation (AF–flutter spectrum).
- 💓 Usually originates in the right atrium (cavotricuspid isthmus-dependent circuit).
🧬 Aetiology
- 🔁 Macro-reentrant arrhythmia (classically cavotricuspid isthmus dependent).
- ❤️ Structural heart disease: IHD, hypertension, valvular disease, cardiomyopathy.
- 🌬️ Systemic triggers: COPD, hyperthyroidism, infection, alcohol (“holiday heart” 🍷).
- 🛠️ Post-cardiac surgery or prior ablation → atypical flutter.
📊 Types of Atrial Flutter
| Type | Characteristics | Clinical Notes |
|---|---|---|
| Typical (CTI-dependent) | Re-entry around tricuspid annulus via cavotricuspid isthmus | Most common; highly amenable to catheter ablation 🔥 |
| Atypical | Non–isthmus dependent circuits (often scar-related) | Seen post-surgery/ablation; requires complex mapping |
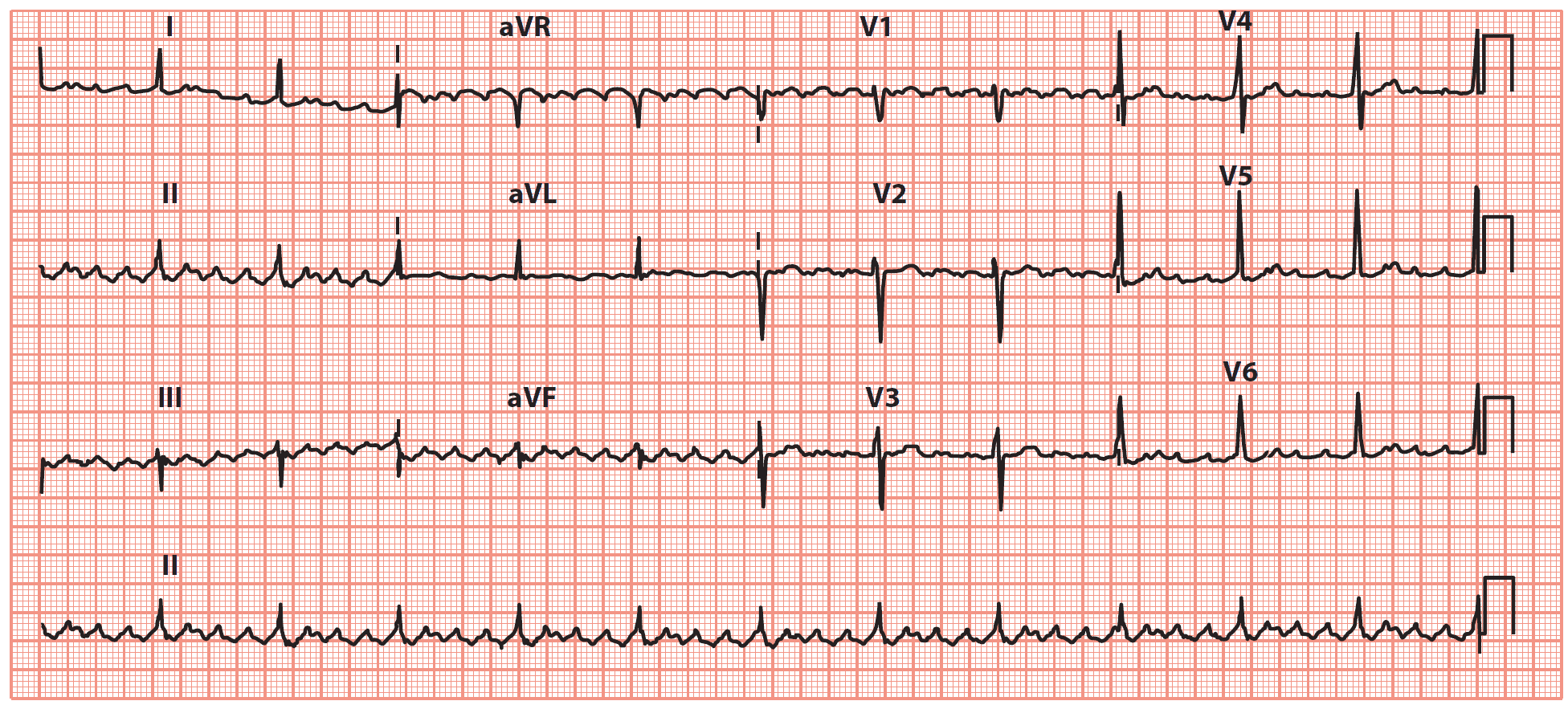
📈 ECG Findings
- 🪚 Sawtooth flutter waves, best seen in leads II, III, aVF.
- ⚡ 2:1 AV conduction → ventricular rate ~150 bpm (common).
- 🚨 1:1 conduction → ventricular rate 250–300 bpm (life-threatening).
- 💉 Adenosine or vagal manoeuvres may unmask flutter waves.

🤒 Clinical Presentation
- 💓 Palpitations, fatigue, dyspnoea, dizziness.
- 🧘 May be asymptomatic if rate controlled.
- 🚨 Severe cases: hypotension, syncope, acute heart failure.
🔬 Investigations
- 🧪 Bloods: FBC, U&E, Mg²⁺, TFTs, CRP, troponin.
- 📈 ECG: diagnostic (flutter waves + conduction pattern).
- 🩻 Echocardiography: assess LV function, atrial size, valvular disease.
- 📟 Holter monitor: paroxysmal detection.
- 💉 Adenosine: diagnostic (transient AV block reveals flutter waves).
⚡ Acute Management (NICE NG196)
- 🚨 Haemodynamically unstable: Immediate synchronized DC cardioversion.
- 🧘 Stable: Rate control first-line (β-blocker or rate-limiting CCB).
- ⏱️ Consider early cardioversion if onset <48h or patient anticoagulated.
🎛️ Rate Control
- β-blockers (e.g. bisoprolol) 👍
- Rate-limiting CCBs (diltiazem/verapamil) 👍
- Digoxin useful in sedentary patients or heart failure ⚠️ (less effective in exertion)
🔄 Rhythm Control
- ⚡ Electrical cardioversion – rapid and effective.
- 💊 Flecainide (ONLY if no structural heart disease) + AV nodal blocker.
- 💊 Amiodarone reserved for structural heart disease or refractory cases.
🔥 Catheter Ablation
- 🎯 First-line definitive therapy for typical atrial flutter.
- 📈 Success rate >90%; low recurrence.
- Reduces need for long-term antiarrhythmic drugs.
🛡️ Anticoagulation (NICE NG196)
- 📊 Use CHA₂DS₂-VASc score (same as AF).
- 💊 DOACs first-line (apixaban, rivaroxaban, dabigatran, edoxaban).
- ⚖️ Warfarin if mechanical valve or moderate–severe mitral stenosis.
- ❌ Do NOT use aspirin monotherapy for stroke prevention.
🚫 Contraindications / Caution
- ❌ Flecainide in structural heart disease or IHD.
- ❌ Non-DHP CCBs in decompensated systolic heart failure.
- ⚠️ Excess β-blockade → bradycardia, hypotension.
- ⚠️ Antiarrhythmics without AV nodal blockade → risk of 1:1 conduction ⚡
📊 Rate vs Rhythm Control
| Scenario | Preferred Strategy | Rationale |
|---|---|---|
| 🚨 Unstable | Immediate DC cardioversion | Life-saving; do not delay |
| 😷 Symptomatic stable | Rate control → consider rhythm control | Stabilise first, then restore sinus rhythm |
| 🔁 Recurrent flutter | Catheter ablation | Definitive, high success |
| 👴 Older/comorbid | Rate control + anticoagulation | Avoid drug toxicity; stroke prevention key |
🩺 Case-Based Learning
- Case 1: 66M, HR 150 → typical flutter. → β-blocker → consider cardioversion → ablation. 🧠
- Case 2: 78F, HF + flutter. → Digoxin + diuretics → anticoagulate → consider ablation. ❤️
- Case 3: 70M, HR 280, hypotensive. → 🚨 Immediate DC cardioversion. ⚡
🌱 Lifestyle & Risk Factor Management
- 🚭 Smoking cessation
- 🍷 Reduce alcohol intake
- ⚖️ Weight optimisation
- 💊 Treat HTN, thyroid disease, COPD
📚 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery