
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
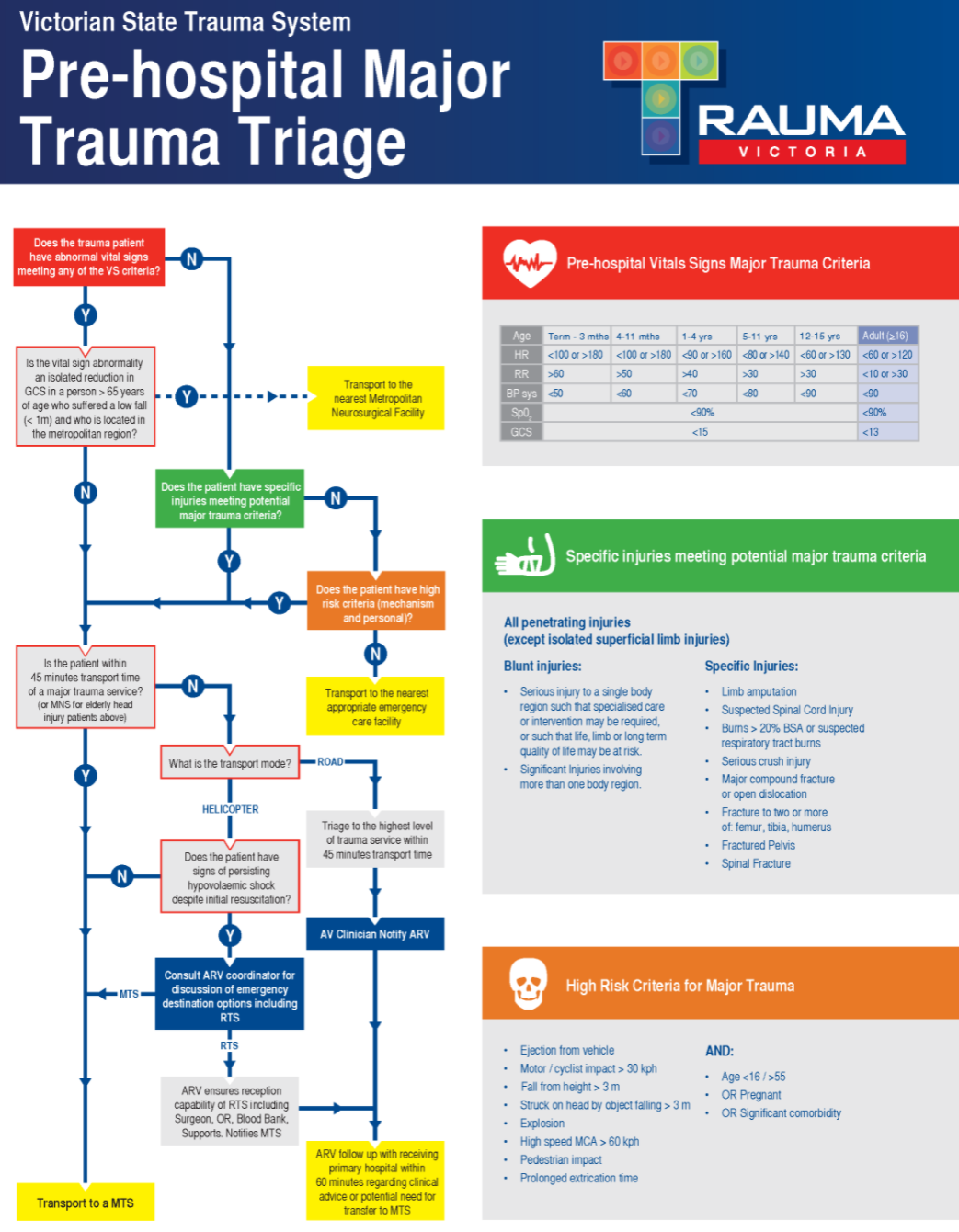
Trauma:Prehospital
Related Subjects: |Initial Trauma Assessment and Management |Thoracic Trauma Assessment and Management |Flail Chest Rib fractures |Resuscitative Thoracotomy |Haemorrhage control |Traumatic Head/Brain Injury |Traumatic Cardiac Arrest |Abdominal trauma |Tranexamic Acid |Silver Trauma |Cauda Equina
🚑 Introduction
- Pre-hospital trauma care is a rapidly developing specialty, combining clinical skills with rescue safety principles.
- ⚠️ Safety first: Rescuer safety always precedes patient care.
- Framework: MARCH (Massive haemorrhage → Airway → Respiration → Circulation → Head/Disability).
🚨 Arrival at the Scene
- 🚗 Position vehicle to protect the scene & warn other traffic (beacons/lights).
- 👷♂️ Safe exit & hazard check before approaching patient.
- 🦺 PPE: fire-retardant overalls, boots with toecaps, gloves, helmet, and eye protection.
- 🔥 Liaise with fire service to make the scene safe before patient contact.
- 🔍 "Read the wreckage": mechanism of injury predicts likely trauma pattern.
- 📡 Early communication → mobilises resources faster.
- 🚻 Triage if multiple casualties: prioritise based on physiology and survivability.
- 🚒 Fire service may be needed for access/extrication planning.
🌟 Exam Pearl: In major incidents, use Sieve & Sort triage. Immediate priority = airway obstruction, catastrophic haemorrhage, or compromised breathing.
🩸 Primary Survey – MARCH
- M = Massive Haemorrhage
- Direct pressure → elevation → indirect pressure → wound packing → tourniquet → haemostatic agents.
- Chest/abdominal bleeding ➝ rapid transfer to hospital (prehospital control not possible).
- A = Airway + C-spine
- Manual in-line stabilisation (jaw thrust, avoid head tilt/chin lift).
- Adjuncts: oropharyngeal/nasopharyngeal airway, supraglottic device if trained.
- Definitive: Intubation if feasible.
- Rescue: Surgical airway (scalpel–bougie–tube or Melker kit) if unable to ventilate.
- R = Respiration
- High-flow O₂ as soon as safe.
- Seal open/sucking chest wounds.
- Needle decompression (2nd ICS mid-clavicular or 5th ICS anterior axillary) → chest drain.
- Reassess RR, SaO₂, trachea, percussion note, chest expansion.
- C = Circulation
- IV/IO access (do not delay transfer for IV attempts).
- Permissive hypotension: Titrate fluids to palpable radial pulse (or carotid in chest trauma).
- 250ml boluses isotonic saline if shocked. Prefer blood products if available (MHP).
- Target higher BP if head injury (maintain CPP).
- H = Head / Disability
- Assume C-spine injury until excluded → collar + blocks + tape.
- Rapidly reverse hypoxia & hypotension.
- Agitated/unconscious ➝ secure airway, prevent aspiration.
- Transport urgently to neurosurgical centre.
👥 Trauma Team Activation Criteria
- SBP < 90 mmHg
- RR < 10 or > 30
- GCS < 12 with torso/extremity trauma
- Pregnant > 20 weeks with abnormal foetal HR
- Amputation proximal to elbow/knee
- ≥2 proximal long bone fractures
- Suspected spinal cord injury
- Severe airway-compromising maxillofacial trauma
- Burns > 15% TBSA
- Gunshot proximal to knee/elbow or trunk/head/neck
- Ejection from vehicle / pedestrian thrown
- Fall > 6 m
- ≥3 major trauma patients arriving simultaneously
- Or: Emergency doctor judgement
📝 Key Principle: In trauma, fix what kills first. Control haemorrhage, oxygenate, decompress chest, then stabilise for transfer. Definitive care is in hospital.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery