
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Acute and Chronic Gout ✅
Related Subjects: |Rheumatoid arthritis |Systemic Sclerosis (Scleroderma) |RA vs OA |Acute and Chronic Gout |Calcium Pyrophosphate Deposition (Pseudogout) |Hyperuricaemia |Allopurinol |Rasburicase |Lesch-Nyhan syndrome
⚠️ It is very rare for acute gout to occur in a rheumatoid joint (due to local anti-inflammatory environment). 👉 Continue treatment until 1–2 days after the attack has resolved and ensure follow-up. 🚑 Admit if septic arthritis is suspected (always exclude this via joint aspiration if possible). 📌 Remember: serum urate may be normal during an acute attack, so repeat 2+ weeks later (NICE NG219).
| Acute Gout Flare – Confirm diagnosis. Exclude Infection. Treatment (NICE NG219) |
|---|
Individualise choice (e.g. steroids preferred in CKD/cardiac disease where NSAIDs riskier). Review response in 48–72 h. Refer if refractory or diagnostic uncertainty. |
🔎 About
- Gout is the most common inflammatory arthritis, caused by deposition of monosodium urate monohydrate crystals in joints/soft tissues.
- Chronic hyperuricaemia (serum urate >360 µmol/L) leads to recurrent flares, tophi, chronic gouty arthritis, urolithiasis, and urate nephropathy.
- Common precipitants in elderly: thiazides, low-dose aspirin, ciclosporin, dehydration, alcohol binge, surgery, or dietary purines.
🧬 Aetiology
- Hyperuricaemia from overproduction (<10%; e.g., purine disorders, haematological malignancy, tumour lysis) or underexcretion (>90%; genetic, CKD, drugs).
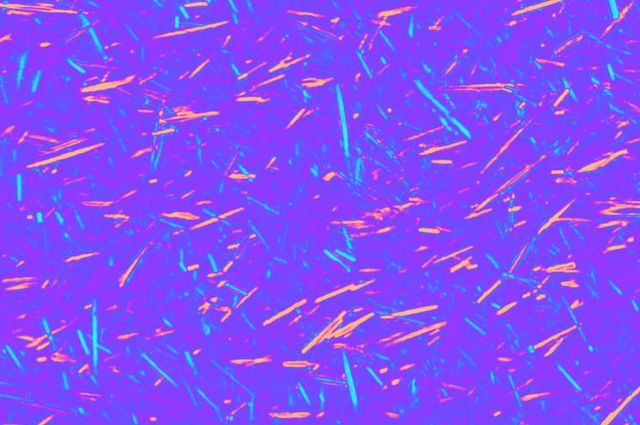
- Crystals: needle-shaped, strongly negatively birefringent under polarised light microscopy.
- Classically affects 1st MTP joint (podagra; ~50% first attacks).
- Precipitating drugs: thiazides, ciclosporin, low-dose aspirin (<325 mg), pyrazinamide.
⚡ Effects of Hyperuricaemia
- Asymptomatic hyperuricaemia (common; no treatment unless very high risk).
- Acute gouty arthritis (mono/polyarticular flares).
- Chronic tophaceous gout (tophi, joint damage, deformity).
- Renal: urate nephrolithiasis (~20%), chronic urate nephropathy → CKD.
📊 Epidemiology
- Male predominance (M:F ≈ 3–10:1; postmenopausal women rise).
- Prevalence ~2.5–3.2% in UK adults (higher in men >40, obesity, metabolic syndrome).
- Lifestyle factors: alcohol (beer/spirits), obesity, high-purine diet (red meat, seafood), fructose-sweetened drinks.
🦶 Podagra – 1st MTP joint (classic site)

🏔️ Chronic Tophaceous Gout

🔬 Urate Crystals

⚠️ Risk Factors
- Male sex, age >40 (postmenopausal women), obesity, metabolic syndrome (hypertension, diabetes, dyslipidaemia).
- CKD, diuretics, low-dose aspirin, alcohol excess, high-purine diet.
- Genetic predisposition (e.g., SLC2A9/ABCG2 variants impair excretion).
- Rare: Lesch-Nyhan (HGPRT deficiency), tumour lysis, lead poisoning (saturnine gout).
🔺 Causes of Excess Urate
- Reduced excretion: CKD, thiazides/loop diuretics, low-dose aspirin, hypertension, lactic acidosis (alcohol/starvation), hypothyroidism, lead toxicity.
- Overproduction: HGPRT deficiency, PRPP synthetase overactivity, myeloproliferative/lymphoproliferative disorders, psoriasis, extreme exercise.
🩺 Clinical Presentation
- Sudden onset (often nocturnal), severe pain maximal in 6–12 hours, swelling, erythema, extreme tenderness (may mimic cellulitis/septic joint).
- Attack duration: 5–14 days untreated; systemic features (fever, malaise, ↑CRP/WCC).
- Polyarticular in chronic/untreated cases.
🚨 Complications
- Chronic tophi → visible/subcutaneous lumps, joint destruction/deformity, disability.
- Urate nephrolithiasis (~20%).
- Chronic urate nephropathy → progressive CKD.
🧪 Investigations (NICE NG219 Compliant)
- Bloods: FBC, U&E (CKD screen), CRP/ESR (raised in flare), serum urate (may normalise in flare → repeat ≥2 weeks post-flare).
- Joint aspiration: Gold standard (negatively birefringent needle crystals; exclude septic arthritis via Gram stain/culture).
- Radiology: Plain X-ray (punched-out erosions with overhanging edges, soft-tissue tophi); dual-energy CT (urate deposits) if available.
💊 Management (NICE NG219 Compliant)
- Acute flare: First Line. Rest, elevate, ice, analgesia.
- NSAID e.g. naproxen 500 mg BD or indomethacin 50 mg TDS + PPI if GI risk
- Colchicine low-dose: 500 µg BD–TDS (max 6 mg/course; caution diarrhoea/CKD)
- Oral corticosteroid e.g. prednisolone 15–30 mg OD for 3–5 days (no taper needed)
- Always exclude septic arthritis (aspiration if possible; admit if suspected).
- Do not stop ULT (allopurinol/febuxostat) during flare.
- Information & support: Educate on chronic nature, treatable, importance of adherence; provide written info.
- Diet & lifestyle: Advise weight loss if overweight, limit alcohol (esp. beer/spirits), avoid dehydration, reduce purine-rich foods (red meat/offal, seafood), limit sugary drinks.
- Long-term ULT:
- Offer to all with: recurrent flares (≥2/year), tophi, chronic gouty arthritis, joint damage, CKD ≥3, urolithiasis, or very high urate.
- Treat-to-target: Start low-dose allopurinol (100 mg OD; lower in CKD) or febuxostat (80 mg OD); titrate to target serum urate <360 µmol/L (<300 µmol/L if tophi/chronic damage).
- Prophylaxis: Colchicine (or NSAID/low-dose steroid) for ≥3–6 months when initiating ULT to prevent mobilisation flares.
- Febuxostat if allopurinol intolerant/fails; pegloticase (IV uricase) for severe refractory tophaceous gout (specialist only).
- Monitoring: Serum urate every 4 weeks during titration, then 6-monthly; renal function; flares/tophi.
- Referral to specialist: Diagnostic uncertainty, refractory gout, severe tophaceous disease, CKD complicating management.
📚 References (Current as of March 2026)
- NICE NG219 – Gout: diagnosis and management (2022; current)
- BSR Guideline for the Management of Gout (2017; complementary but superseded in UK by NG219)
- ACR 2020 Guideline for the Management of Gout (complementary international reference).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery