
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Hypoglycaemia
Related Subjects: Type 1 DM |Type 2 DM |Diabetes in Pregnancy |HbA1c |Diabetic Ketoacidosis (DKA) Adults |Hyperglycaemic Hyperosmolar State (HHS) |Diabetic Nephropathy |Diabetic Retinopathy |Diabetic Neuropathy |Diabetic Amyotrophy |Maturity Onset Diabetes of the Young (MODY) |Diabetes: Complications |Hypoglycaemia |Gold Score: Hypoglycaemia Awareness in Type 1 Diabetes
| 🚨 Hypoglycaemia Urgent Management. Also see
|Gold Score: Hypoglycaemia Awareness in Type 1 Diabetes
Capillary or Plasma Glucose < 3–4 mmol/L (≈72 mg/dL) |
|---|
|
📖 Introduction
- Hypoglycaemia is potentially fatal - delayed treatment risks irreversible brain injury.
- Most common cause: 💉 Insulin or sulfonylureas (missed meals, OD, deliberate self-harm).
⚠️ Think broadly: Addison’s disease, liver failure, alcohol binge without food, insulinoma, pituitary disease, quinine, severe sepsis, malaria.
🧪 Clinical Features
- 🤯 Autonomic: Sweating, tremor, palpitations, hunger, anxiety.
- 🧠 Neuroglycopenic: Confusion, odd behaviour, slurred speech, seizures, coma.
- 💥 May mimic stroke, seizure, delirium → always check CBG!
🧾 Whipple’s Triad
- Compatible symptoms/signs of hypoglycaemia.
- Documented low plasma glucose.
- Resolution after glucose correction.
🔍 Investigations
- Confirm lab glucose + CBG.
- Insulin & C-peptide (to distinguish endogenous vs exogenous insulin use).
- Consider: LFTs, renal profile, cortisol/ACTH, ±72-hour fast if unexplained.
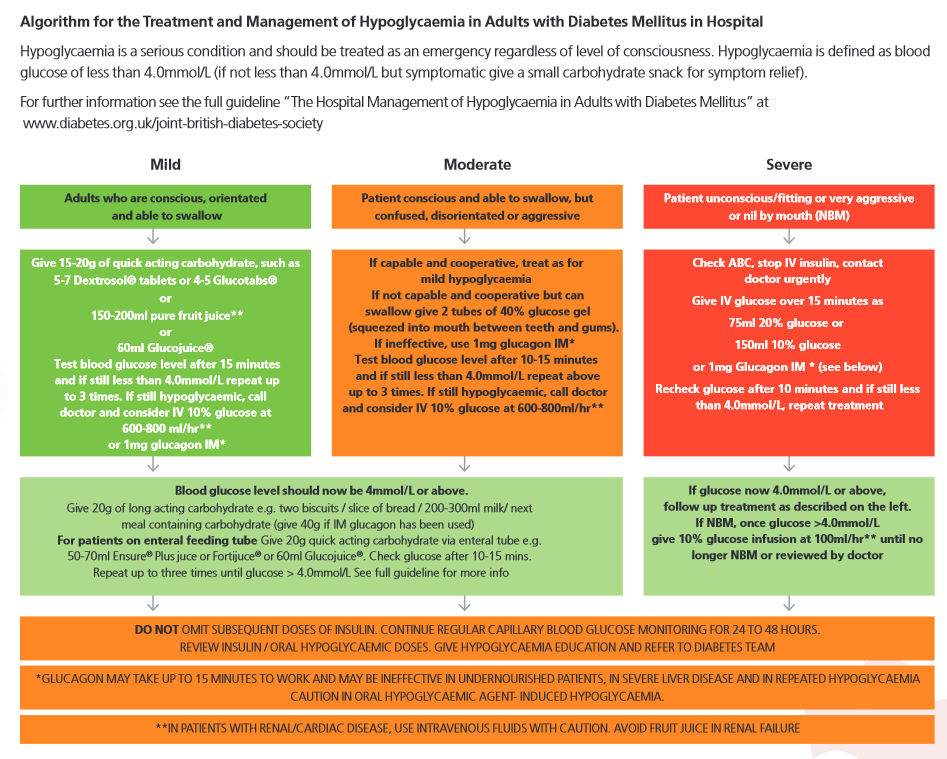
💊 Management (Stepwise)
- 📏 Measure CBG: <3–4 mmol/L → act immediately.
- 🥤 If cooperative: 15–20 g rapid sugar (e.g., 150 mL pure juice). Recheck in 10–15 min. Repeat ×3 if still <4.
- 🍯 If uncooperative but safe swallow: 2 tubes of 40% glucose gel (e.g., Glucogel) buccally.
- 💉 If unable to swallow/unconscious:
- IV 150 mL 10% glucose (or 20/50% equivalents) → recheck after 10 min.
- IM/SC glucagon 1 mg (intranasal 3 mg if available).
- ⏳ Prolonged hypoglycaemia: IV infusion 10% glucose; monitor closely.
- 🍺 Alcohol/malnutrition: Give IV thiamine (Pabrinex) with glucose.
- 🔄 Aftercare: Prevent recurrence → adjust insulin/meds, review diet, diabetes specialist input.
📊 Causes (Mnemonics)
- Exogenous: Insulin, sulfonylureas, quinine, alcohol binge.
- Endogenous: Insulinoma, Addison’s, pituitary failure, severe sepsis.
- Misc: Critical illness, malnutrition, bodybuilders misusing insulin.
📑 References
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery