Related Subjects:
|Episcleritis
|Scleritis
|Assessing a Red eye
|Acute Angle Closure Glaucoma
|Allergic and Infective Conjunctivitis
|Anterior and Posterior Uveitis
|Atropine Sulfate
|Herpes simplex keratitis (HSK)
|Acute Blepharitis
|Chalazion
🍇 “Uveitis” comes from the Latin word uva, meaning grape, because the inflamed uveal tract was thought to resemble a grape’s dark colour. 🚨 If there has been recent intraocular surgery (for example cataract surgery) or an intravitreal injection, always consider endophthalmitis as a cause of pain, photophobia, and reduced vision - this needs same-day ophthalmology assessment.
👁️ About
- 🔥 Uveitis is inflammation of the uveal tract: the iris, ciliary body, and choroid.
- 🧩 It may be caused by trauma, iatrogenic causes, infection, drugs, systemic autoimmune disease, or may be idiopathic.
- ⚠️ Anterior uveitis is the most common type and can cause significant pain, photophobia, and potentially sight-threatening complications if untreated.
📊 Epidemiology
- ❓ More than 50% of cases are idiopathic.
- 👥 It can occur at any age, but is common in working-age adults.
- 👁️ Anterior uveitis is the most common form of uveitis.
🗂️ Types
- Anterior uveitis 👁️: involves the iris and/or ciliary body (iritis, cyclitis, iridocyclitis).
- Intermediate uveitis 🌫️: mainly involves the vitreous and peripheral retina.
- Posterior uveitis 🧠: affects the choroid and/or retina (for example choroiditis, retinitis, chorioretinitis, retinal vasculitis).
- Panuveitis 🌍: inflammation affecting the whole uveal tract.
🧬 Aetiology
- Idiopathic ❔: common, especially in anterior uveitis.
- HLA-B27-associated disease 🦴: ankylosing spondylitis, psoriatic arthritis, reactive arthritis, inflammatory bowel disease.
- Paediatric / rheumatological causes 🧒: juvenile idiopathic arthritis, Behçet’s disease, sarcoidosis, vasculitis.
- Infective causes 🦠: herpes simplex virus, varicella-zoster virus, CMV, syphilis, TB, toxoplasmosis, Lyme disease, leptospirosis, brucellosis.
- Systemic inflammatory disease 🔥: sarcoidosis, Crohn’s disease, ulcerative colitis, multiple sclerosis.
- Trauma / iatrogenic 🔧: blunt trauma, penetrating injury, eye surgery, intravitreal procedures.
- Masquerade / rare causes 🎭: intraocular lymphoma and other neoplastic causes.
🩺 Clinical Features
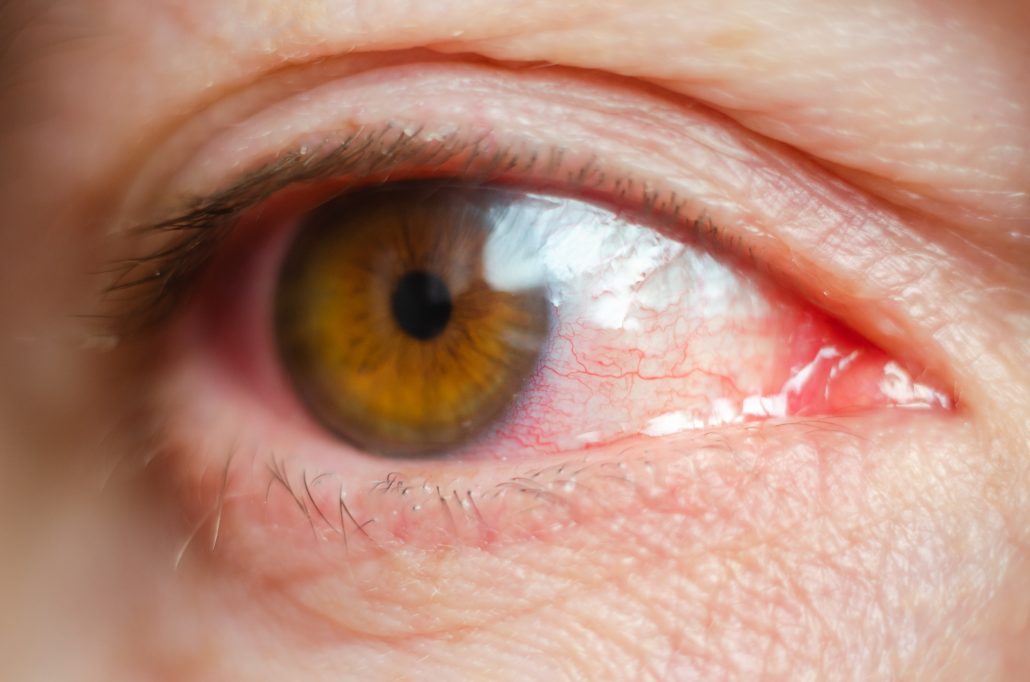
- 😖 Ocular pain, often aching in nature.
- 💡 Photophobia, especially marked in anterior uveitis.
- 💧 Tearing / watering.
- 🔴 Red eye, often most intense around the limbus (ciliary flush).
- 👁️ Blurred vision or reduced visual acuity.
- 🔹 Miosis (small pupil) from iris spasm.
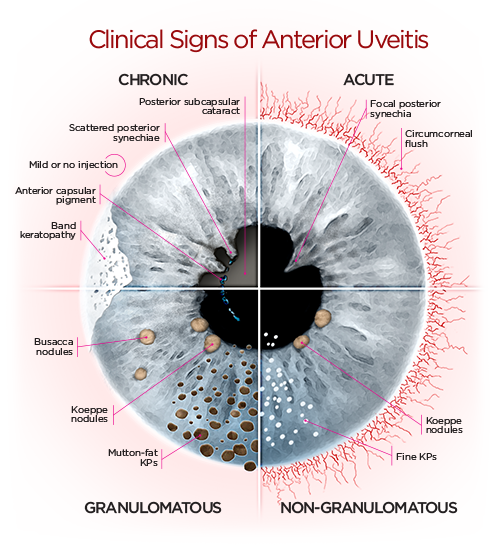
- 🌫️ Cells and flare in the anterior chamber.
- 🧪 Keratic precipitates, posterior synechiae, or occasionally a hypopyon.
- 📈 Intraocular pressure may be raised or low, depending on the cause and stage.
- 🧴 Always check for corneal staining and consider keratitis or trauma if the history suggests it.
🔍 Investigations
- Slit-lamp examination 🔬: looks for cells and flare, keratic precipitates, synechiae, hypopyon, and corneal involvement.
- Visual acuity 👓: should be documented in all patients.
- Intraocular pressure 📏: important to check, especially if glaucoma is a differential.
- Fluorescein staining 💧: helps exclude corneal ulceration, abrasion, or keratitis.
- PCR / aqueous or vitreous sampling 🧫: may be useful in suspected viral uveitis or acute retinal necrosis.
- Systemic work-up 🩸: guided by history and examination; may include FBC, ESR/CRP, HLA-B27, syphilis serology, TB testing, and chest imaging if sarcoid or TB is suspected.
- Ocular imaging 🖥️: OCT, fundus photography, fluorescein angiography, or B-scan ultrasound for posterior/intermediate disease.
⚖️ Differentials
- Endophthalmitis 🚨: especially after surgery or intravitreal injection.
- Keratitis 🦠: bacterial, viral, fungal, or contact-lens related.
- Acute angle-closure glaucoma 🔺: painful red eye with headache, nausea, haloes, and raised IOP.
- Corneal abrasion or foreign body 🧲.
- Scleritis 🔥: severe deep boring pain, often associated with systemic inflammatory disease.
- Chemical injury ⚗️.
⚠️ Complications
- Posterior synechiae 🧷.
- Secondary glaucoma 📈.
- Cataract 👓: from inflammation or steroid treatment.
- Cystoid macular oedema 🌊.
- Band keratopathy 🪨.
- Corneal scarring 🩹.
- Permanent visual loss 🚫👁️ if severe, recurrent, or undertreated.
🛠️ Management
- 👨⚕️ Ophthalmology referral is essential for suspected uveitis.
- ⏰ Arrange urgent / same-day ophthalmology review if there is severe pain, reduced vision, hypopyon, corneal involvement, or suspicion of endophthalmitis.
- 🚫 In primary care, do not usually start treatment unless specifically advised by an ophthalmologist.
- Anterior uveitis 👁️ (after ophthalmology review) is commonly treated with:
- 💧 Topical corticosteroids (for example prednisolone eye drops), tapered according to response.
- 🌀 Cycloplegic / mydriatic drops (for example cyclopentolate, homatropine, or atropine) to reduce ciliary spasm, relieve pain, and prevent posterior synechiae.
- Infective causes 🦠 require treatment of the underlying pathogen, for example antiviral therapy in herpetic disease.
- Posterior, intermediate, or severe disease 💥 may require systemic steroids, periocular/intravitreal steroids, or steroid-sparing immunosuppression / biologics under specialist care.
- 🕶️ Supportive measures include sunglasses, reduced bright-light exposure, and advice to seek urgent reassessment if vision worsens.
🚑 Red Flags
- Recent cataract surgery or intravitreal injection + pain / photophobia / reduced vision.
- Loss of vision or rapidly worsening visual acuity.
- Hypopyon.
- Corneal opacity, ulcer, or staining.
- Markedly raised IOP or features suggesting acute angle-closure glaucoma.
- History of contact lens wear with painful red eye.
💡 Teaching Points
- Anterior uveitis is a classic cause of the painful photophobic red eye.
- The exam clue is often ciliary flush + consensual photophobia + small pupil.
- Never miss endophthalmitis, keratitis, or acute angle-closure glaucoma in the differential.
- Think systemically: recurrent uveitis may be the first clue to HLA-B27 disease, sarcoidosis, Behçet’s, or infection.
📚 References