
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Brain CT Collection
Calcified Pineal

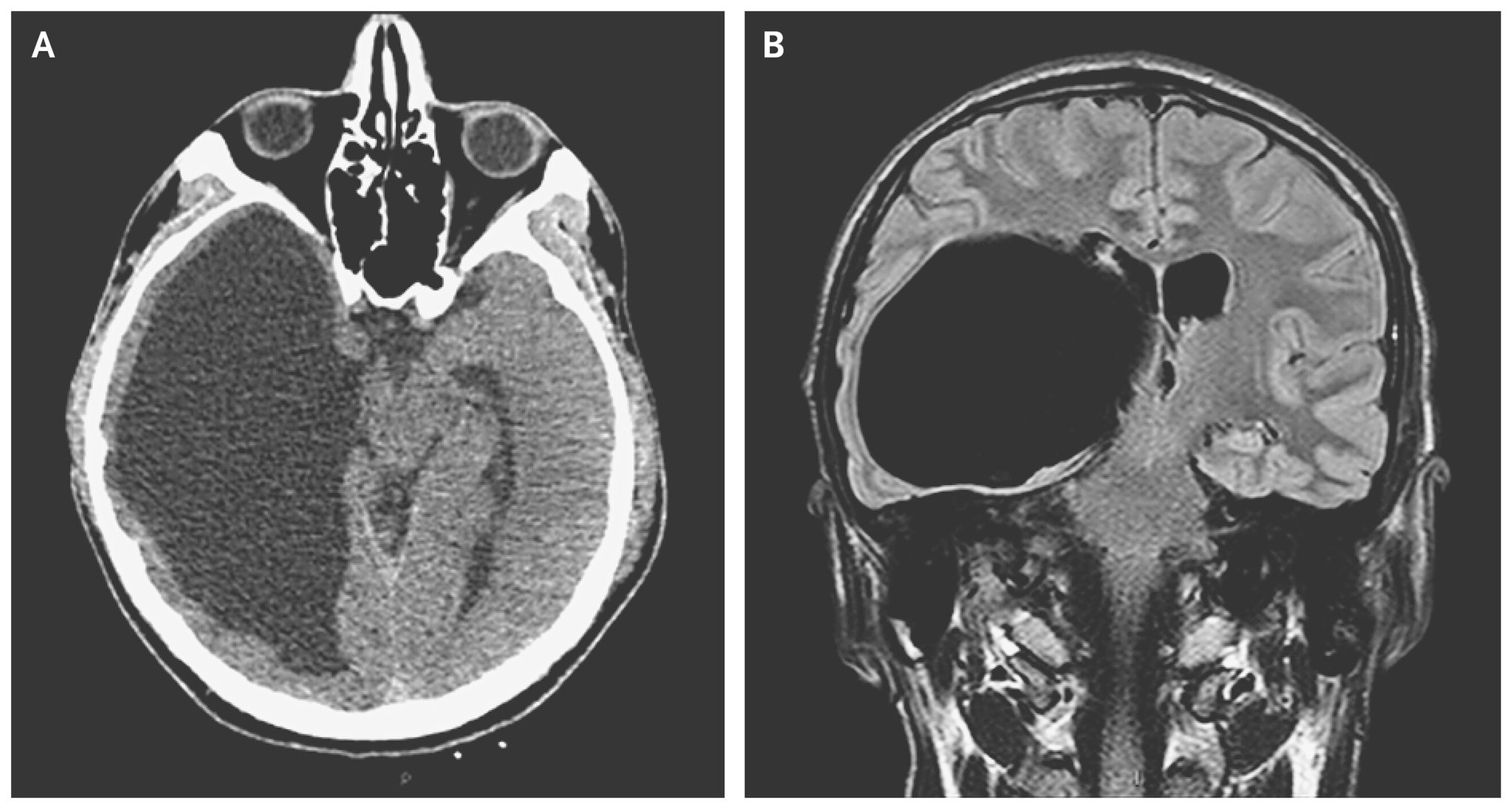
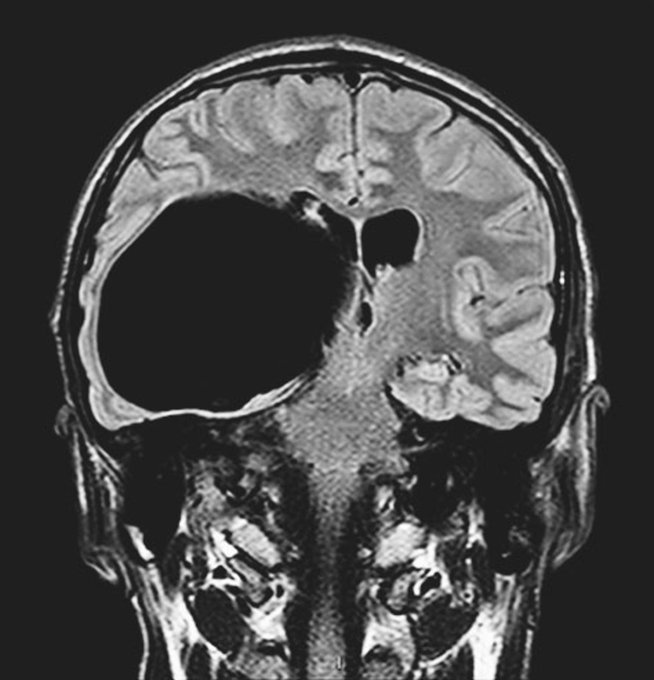
Arachnoid Cyst
🫧 Expected imaging findings:
• Well-circumscribed extra-axial cyst with CSF density on CT and CSF signal on MRI.
• No enhancement with contrast and no restricted diffusion.
• Often causes mass effect (sulcal effacement, midline shift) if large, but no surrounding oedema.
• Common locations: middle cranial fossa, posterior fossa, suprasellar region.
⚠️ Usually incidental; symptomatic cases cause headache, seizures, focal deficits or hydrocephalus.
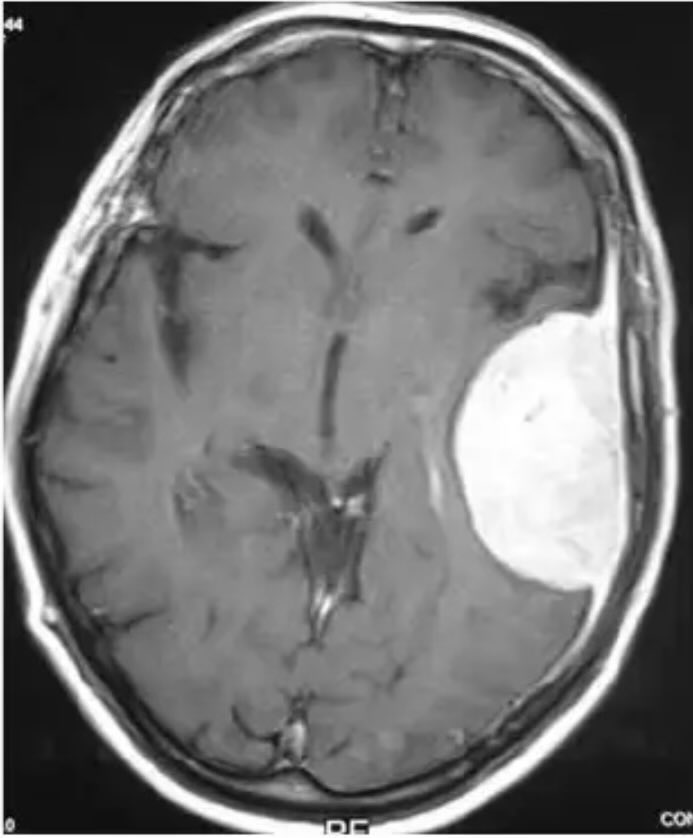
Meningioma
🧠 Expected imaging findings:
• Extra-axial, dural-based mass; often hyperdense on non-contrast CT.
• Vivid homogeneous enhancement post-contrast.
• Classic dural tail sign on MRI/contrast CT.
• May show hyperostosis or calcification adjacent to the lesion.
• Causes mass effect and often vasogenic oedema in underlying brain.
⚠️ Symptoms depend on location (seizures, focal deficit, raised ICP).
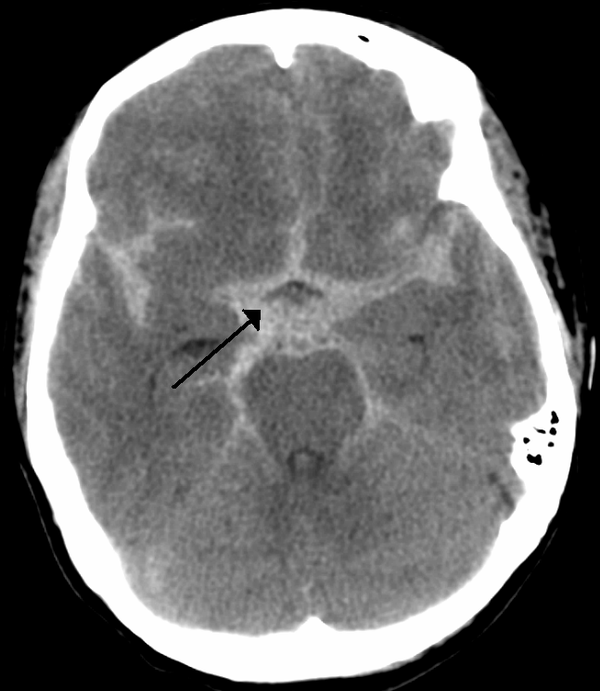
Subarachnoid Haemorrhage
🩸 Expected imaging findings:
• On non-contrast CT: hyperdensity in basal cisterns, sulci, and fissures (“star sign”).
• Blood may layer in the ventricles (intraventricular extension).
• Early CT (first 6–12 hours) is most sensitive; sensitivity falls with time.
• CT angiography may show aneurysm; LP (xanthochromia) if CT negative and suspicion high.
🚨 Clinical clue: thunderclap headache ± meningism, collapse, reduced GCS.
Lung Mets with and without Contrast
🎯 Expected imaging findings:
• Multiple rounded pulmonary nodules of varying size (“cannonball” pattern possible).
• Non-contrast CT shows distribution and calcification; contrast improves mediastinal/hilar assessment and vascular relationships.
• Look for pleural deposits, lymphangitis carcinomatosis (septal thickening), or effusions depending on tumour type.
• Haematogenous spread often gives peripheral, well-defined nodules.
⚠️ Always interpret in clinical context: primary tumour history, weight loss, haemoptysis.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery