Transjugular Intrahepatic portosystemic shunt (TIPS)
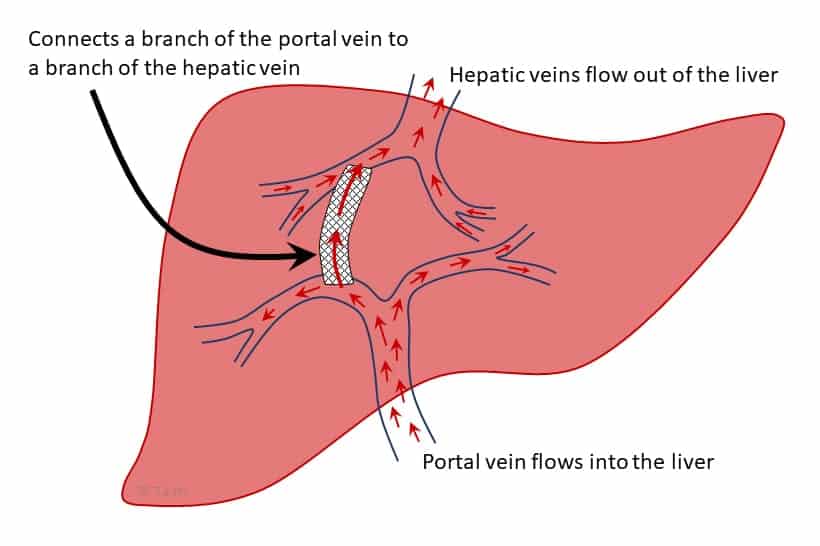
🫀 Transjugular Intrahepatic Portosystemic Shunt (TIPS) is a radiological procedure creating a channel between the portal vein and hepatic vein to relieve portal hypertension. It is mainly used for variceal bleeding and refractory ascites.
🎯 Indications for TIPS
- 🩸 Variceal Bleeding: Refractory/recurrent bleeding not controlled by endoscopy.
- 💧 Refractory Ascites: Resistant to diuretics or requiring repeated paracentesis.
- 🌊 Hepatic Hydrothorax: Pleural effusion due to portal hypertension.
- 🫀 Budd-Chiari Syndrome: Venous outflow obstruction.
- 🩺 Portal Vein Thrombosis: Selected cases to restore flow.
🛠️ Procedure
- Access: Via the internal jugular vein → catheter advanced into hepatic veins.
- Shunt Creation: Needle puncture from hepatic vein into portal vein tract.
- Stent Placement: Maintains portosystemic channel, diverting blood into systemic circulation.
⚙️ Pathophysiology
- Portal Hypertension: Cirrhosis → ↑ portal pressure → varices & ascites.
- TIPS Effect: Reduces portal pressure → ↓ variceal bleed risk & ascites formation.
🚫 Contraindications
- Severe/recurrent hepatic encephalopathy.
- Advanced right heart failure.
- Severe liver failure (Child-Pugh C, MELD >15).
- Active sepsis.
- Extensive portal vein thrombosis.
🦷
Ameloblastoma is a rare, benign but locally aggressive odontogenic tumour arising from the enamel-forming epithelium. Most commonly in the mandible, it can cause significant jaw expansion and deformity if untreated.
📖 About
- Incidence: ~1% of all jaw tumours/cysts.
- Age Group: Peak 30–50 years (but any age possible).
- Location: Mandible (esp. molar & ramus region) >> Maxilla.
- Histopathology: From dental lamina, enamel organ, or odontogenic cyst lining.
🧬 Etiology
- Exact cause uncertain, but linked with:
- Genetic mutations → esp. BRAF V600E.
- Chronic irritation/inflammation.
- Association with impacted teeth/odontogenic cysts.
🩺 Clinical Presentation
- Often asymptomatic in early stages → incidental finding.
- Painless jaw swelling or bony expansion.
- Facial asymmetry & displacement of teeth.
- Root resorption (seen radiographically).
- Occasional pain or paraesthesia if nerves compressed.
🩻 Radiographic Features
- Classic multilocular radiolucency → “soap bubble” or “honeycomb” appearance 💡.
- Well-defined lesion with cortical thinning & expansion.
- Root resorption of adjacent teeth.
🔬 Histological Subtypes
- Conventional (Solid/Multicystic): Most common, aggressive, higher recurrence.
- Unicystic: Single cyst-like lesion, less aggressive, younger patients.
- Peripheral: In soft tissue overlying bone, rare.
- Desmoplastic: Dense stroma with collagenisation.
🛠️ Management
- Surgery = gold standard
- Radical resection (marginal/segmental mandibulectomy) → lower recurrence.
- Curettage/enucleation → higher recurrence, sometimes used for small lesions.
- Reconstruction: May require bone grafts, flaps, or prosthetics for function/appearance.
- Follow-up: Lifelong surveillance → recurrences can appear years later.
📊 Prognosis
- Benign but locally invasive.
- Recurrence:
- 5–15% after wide resection.
- >50% after curettage alone.
- Rare malignant transformation → ameloblastic carcinoma.
📚 References
- Philipsen HP, Reichart PA. J Oral Pathol Med. 2006.
- Speight PM, Takata T. Virchows Arch. 2017.
⚠️ Complications
- 🧠 Hepatic Encephalopathy: Due to toxin bypass → confusion, altered cognition.
- 🩻 Stent Stenosis/Occlusion: May cause recurrence of ascites/bleeding.
- ❤️ Heart Failure: Increased preload can worsen existing cardiac disease.
- 🦠 Infection: Risk during/after procedure.
- 💉 Hemorrhage: Rare but serious intra-procedural bleeding.
🩺 Post-Procedural Care
- Monitor closely for encephalopathy & cardiac decompensation.
- Follow-up Doppler ultrasound (1–3 months, then 6-monthly) to assess patency.
- Lactulose/rifaximin prophylaxis for encephalopathy risk.
- Diuretics may still be required for ascites control.
📊 Prognosis
- Excellent for controlling variceal bleeding & refractory ascites.
- Outcome depends heavily on underlying liver function.
- MELD >15 = poorer prognosis → transplant referral considered.
🔄 Alternative Treatments
- Endoscopic band ligation for varices.
- Large-volume paracentesis for ascites.
- Liver transplantation = definitive cure for advanced cirrhosis.
✅ Conclusion
TIPS is a powerful tool for portal hypertension complications. Careful patient selection, complication monitoring, and long-term follow-up (including Doppler surveillance) are essential to optimise outcomes.
