Von Willebrand Disease
Related Subjects:
|Sideroblastic Anaemia
|Splenectomy
|Blood Products - Platelets
|Von Willebrand Disease
Patients with von Willebrand disease (vWD) often present with mucosal bleeding (e.g. epistaxis, menorrhagia, dental/surgical bleeding). ⚠️ Avoid aspirin & NSAIDs as they worsen bleeding.
💊 Tranexamic acid is frequently used to control episodes.
🧾 About
- Most common inherited bleeding disorder (affects both sexes equally).
- Combination of platelet adhesion defect and factor VIII deficiency.
- Usually autosomal dominant (Type 1 & 2), but autosomal recessive in Type 3.
- Gene: vWF gene on chromosome 12.
🧬 Aetiology & Pathophysiology
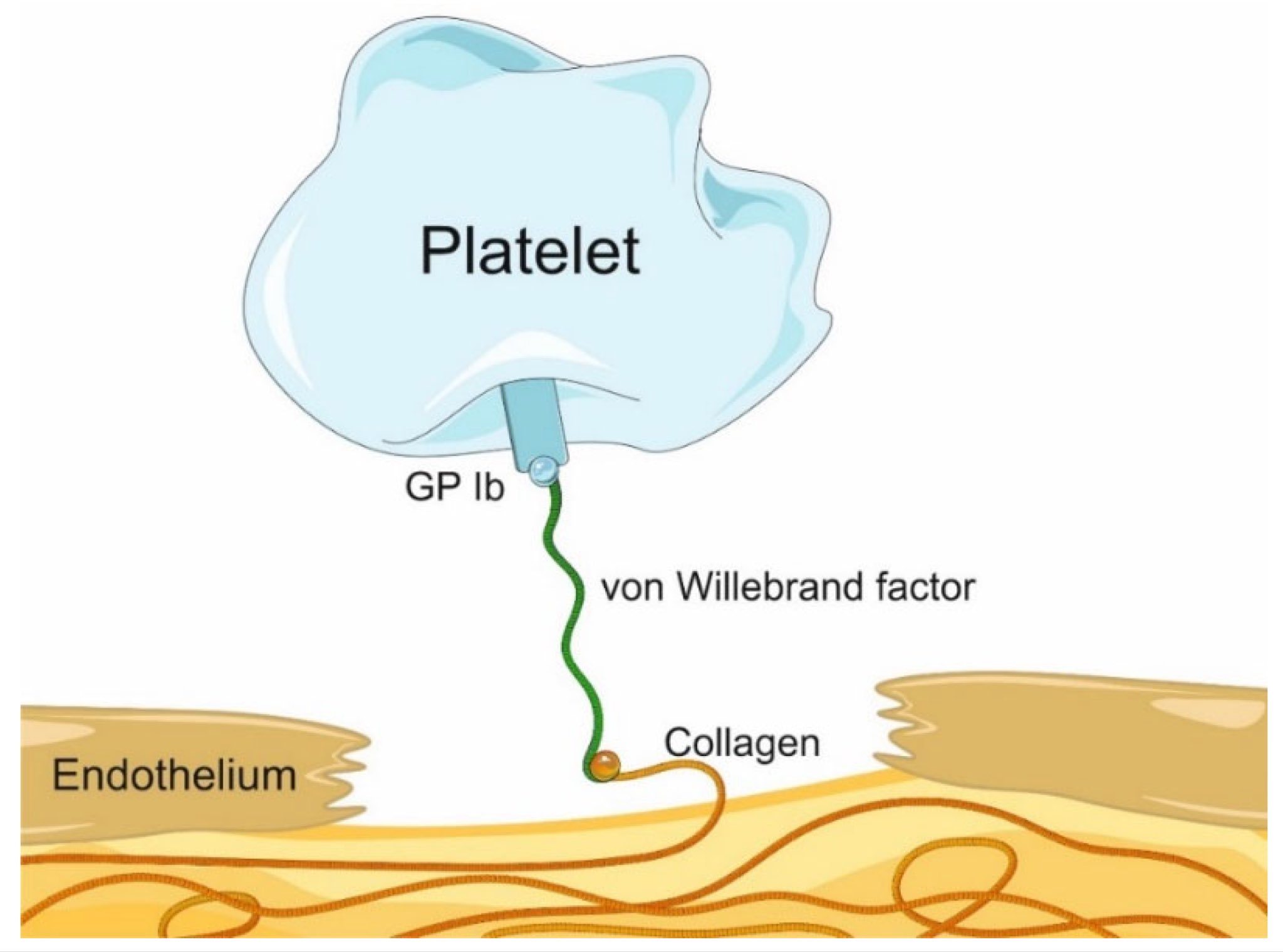
- vWF acts as a "bridge": binds platelets (GpIb) → collagen.
- Also carries and stabilises factor VIII (prevents rapid degradation).
- Deficiency/defect → impaired platelet plug formation + reduced factor VIII.
📊 Types of Von Willebrand Disease
| Type |
Inheritance |
Clinical Features |
Severity |
| Type 1 |
AD |
Mild mucosal bleeding (epistaxis, bruising, menorrhagia) |
Mild (80% of cases) |
| Type 2 (A, B, M, N) |
AD |
Moderate bleeding, qualitative vWF defect |
Moderate |
| Type 3 |
AR |
Severe: mucosal + joint bleeds (hemophilia-like) |
Severe (rare) |
| Acquired |
Secondary |
Seen with autoimmune disease, malignancy, drugs |
Variable |
💡 Exam Tip: Both vWD and Hemophilia A show prolonged APTT, but vWD has mucosal bleeding & prolonged bleeding time, unlike Hemophilia.
🔬 Investigations
| Test | Finding |
|---|
| Bleeding time | Prolonged |
| Platelet count | Normal |
| APTT | Prolonged (↓ Factor VIII) |
| PT | Normal |
| Factor VIII & vWF levels | Low |
| Ristocetin assay | Impaired platelet aggregation (diagnostic) |
💊 Management
- ⚠️ Avoid: Aspirin, NSAIDs, IM injections.
- Tranexamic acid – for mucosal bleeding/menorrhagia.
- Desmopressin (DDAVP) – effective in Types 1 & 2 (↑ release of vWF & VIII from endothelium).
- vWF + Factor VIII concentrate – for severe bleeding or surgery (esp. Type 3).
- Genetic counselling for inherited forms.
Cases - Von Willebrand Disease (vWD)
- Case 1 - Mucocutaneous bleeding 👃: A 15-year-old girl presents with recurrent nosebleeds, easy bruising, and prolonged bleeding after dental extraction. Family history: mother with similar problems. Labs: prolonged APTT, normal platelet count, reduced vWF antigen and ristocetin cofactor activity. Diagnosis: Type 1 vWD (partial quantitative deficiency). Managed with tranexamic acid and desmopressin before procedures.
- Case 2 - Menorrhagia in young woman 🩸: A 22-year-old woman reports very heavy menstrual periods since menarche, requiring double sanitary protection. No other systemic illness. Labs: normal PT, prolonged APTT, low vWF activity, factor VIII borderline low. Diagnosis: Type 2 vWD (qualitative defect). Managed with hormonal therapy for menorrhagia and desmopressin when required.
- Case 3 - Severe bleeding tendency ⚠️: A 10-year-old boy presents with recurrent joint bleeds and prolonged bleeding after minor cuts. Family history negative. Labs: markedly reduced vWF antigen, factor VIII severely reduced. Diagnosis: Type 3 vWD (virtually absent vWF). Managed with vWF-containing factor concentrates and antifibrinolytics.
Teaching Point 🩺: vWD is the commonest inherited bleeding disorder. It causes mucocutaneous bleeding due to impaired platelet adhesion and, in severe cases, reduced factor VIII. Types: Type 1 (partial deficiency), Type 2 (dysfunctional vWF), Type 3 (severe deficiency). Management: tranexamic acid, desmopressin, or vWF concentrates depending on severity.