Related Subjects:
|Colorectal cancer
|Colorectal polyps
|Ulcerative Colitis
|Acute Severe Colitis
|Crohn's disease
|Coeliac disease
|Familial Adenomatous polyposis (FAP)
|Surgical Stomas
🌟 Anti-TNF and other biologics (e.g., infliximab, adalimumab, vedolizumab, ustekinumab) have transformed Crohn’s disease management, improving remission rates and quality of life. They are indicated for moderate–severe active disease or fistulising Crohn’s not controlled by conventional therapy.
📖 About
- 🌱 Crohn's disease = chronic, relapsing, granulomatous inflammatory disorder.
- 🌀 Can affect the GI tract anywhere from mouth → anus.
- 📊 UK incidence: ~5–8/100,000/year; prevalence: 50–80/100,000.
🧬 Aetiology & Risk Factors
- 👩🦳 More common in Caucasian & Jewish populations.
- 🚬 Smoking increases risk ×3–4; cessation improves outcomes.
- 🧪 Genetic: NOD2/CARD15 mutations → often ileal disease.
- 🌍 Environmental: antigen exposure, OCP use, urban lifestyle.
- Family history increases risk.
🔬 Pathology
- Granulomatous, transmural inflammation; deep fissuring ulcers; “cobblestoning” mucosa.
- Patchy “skip lesions” with normal intervening mucosa.
- Fistulae may form: entero-vesical, entero-vaginal, entero-enteric.
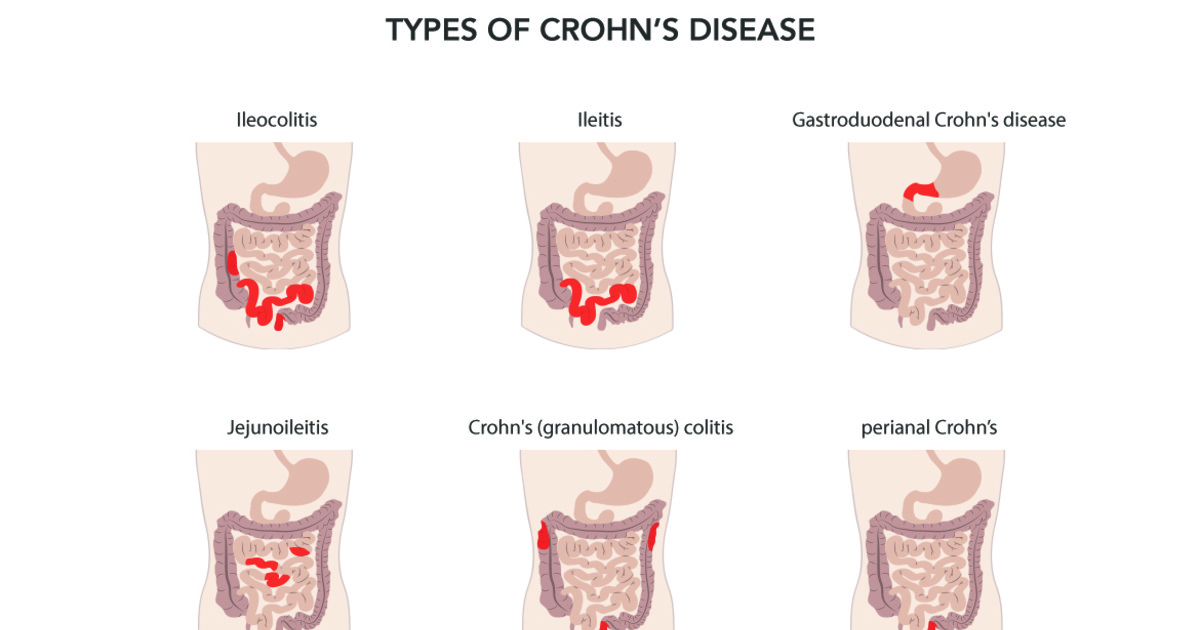
📍 Disease Location
- Terminal ileum: ~90%
- Ileocolonic: 40%
- Small intestine alone: 40%
- Colitis pattern: 20%
- Perianal disease: <10% (rectum often spared)
🩺 Clinical Presentation
- Proximal small bowel: Colicky pain, partial obstruction, weight loss, anorexia.
- Terminal ileum: RLQ pain, steatorrhoea, B12 malabsorption, inflammatory mass.
- Colonic: Diarrhoea ± blood/mucus, abdominal pain.
- Perianal: Skin tags, fistulae, abscesses.
- Systemic: fatigue, anaemia, fever, finger clubbing, aphthous ulcers.
⚠️ Complications
- 👁 Ophthalmic: uveitis, episcleritis
- 🦴 Musculoskeletal: arthropathy, sacroiliitis, ankylosing spondylitis
- 🟤 Skin: erythema nodosum, pyoderma gangrenosum
- 💎 Renal: oxalate stones
- ⬆️ Colonic adenocarcinoma with long-standing colitis
- 🩸 Increased VTE risk
🧻 Harvey-Bradshaw Index: Crohn’s Disease
The Harvey-Bradshaw Index (HBI) is a simple clinical score used to assess Crohn’s disease activity.
It is quicker than the Crohn’s Disease Activity Index and is useful for monitoring symptoms over time.
📋 Components
| Component |
Score |
| General wellbeing yesterday |
Very well = 0; slightly below par = 1; poor = 2; very poor = 3; terrible = 4 |
| Abdominal pain yesterday |
None = 0; mild = 1; moderate = 2; severe = 3 |
| Number of liquid or soft stools yesterday |
1 point per stool |
| Abdominal mass |
None = 0; dubious = 1; definite = 2; definite and tender = 3 |
| Complications |
1 point each |
⚠️ Complications Scored
- Arthralgia
- Uveitis
- Erythema nodosum
- Aphthous ulcers
- Pyoderma gangrenosum
- Anal fissure
- New fistula
- Abscess
📊 Interpretation
| Total HBI score |
Disease activity |
| <5 |
Remission |
| 5–7 |
Mild disease activity |
| 8–16 |
Moderate disease activity |
| >16 |
Severe disease activity |
🧠 Clinical Use
- Used to monitor Crohn’s disease symptoms at clinic review or during a suspected flare.
- Helps track response to treatment over time.
- A fall of around 3 points is often considered a clinically meaningful improvement.
- Should be interpreted alongside CRP, faecal calprotectin, nutrition, weight, imaging, endoscopy and clinical judgement.
⚠️ Important Points
- The HBI is for Crohn’s disease, not ulcerative colitis.
- It measures clinical activity, not mucosal healing.
- A low score does not fully exclude active inflammation, stricturing disease or penetrating complications.
- Severe pain, fever, obstruction, peritonism, abscess, sepsis or significant weight loss should prompt urgent senior review.
🧠 Exam Pearl
- HBI <5 suggests remission; 5–7 mild; 8–16 moderate; >16 severe Crohn’s disease activity.
- Remember the score combines symptoms, stool frequency, abdominal mass and extra-intestinal/perianal complications.
🔎 Investigations
- 🩸 Bloods: Hb, ferritin, B12/folate, ESR/CRP, LFTs, bone profile.
- 💩 Stool: Ova/cysts/parasites; faecal calprotectin (inflammation marker).
- Endoscopy: Ileocolonoscopy + biopsy = gold standard (granulomas if present).
- Imaging:
- AXR: Obstruction
- Barium follow-through: “String sign of Kantor”
- CT enterography: Activity + complications
- MRI pelvis: Perianal fistulae
- Antibodies: ASCA +ve in ~60%
🔄 Differential Diagnosis
- Tuberculosis enteritis
- Yersinia infection
- Other ileitis causes: vasculitis, lymphoma
🔍 Comparison: Crohn’s Disease vs Ulcerative Colitis
| Feature | 🌱 Crohn’s Disease | 🔥 Ulcerative Colitis |
| Distribution | Anywhere mouth → anus, skip lesions | Starts in rectum, continuous proximally |
| Depth of Inflammation | Transmural | Mucosa + submucosa only |
| Histology | Non-caseating granulomas, fissures | Crypt abscesses, mucosal ulceration, no granulomas |
| Appearance | “Cobblestone”, thick bowel wall, strictures, fistulas | Red, friable mucosa, pseudopolyps |
| Symptoms | RLQ pain, diarrhoea ± blood, weight loss, perianal disease | Bloody diarrhoea, urgency, tenesmus, LLQ pain |
| Smoking | 🚬 Risk factor | 🚭 Protective |
| Extra-intestinal | Renal stones, gallstones, B12 deficiency | PSC, ↑ colorectal cancer risk |
| Fistula/Stricture | ✅ Common | ❌ Rare |
| Surgery | Not curative, recurrence common | Curative |
| Cancer risk | ↑ with colonic involvement | High with pancolitis/PSC |
💡 Teaching Tip:
- Crohn’s → Cobblestone, Complete wall, Complications (fistulae/strictures)
- UC → starts in Ulcerated rectum, continuous, mucosal only, curable with colectomy
💊 Management (Stepwise)
- Mild: Oral/rectal 5-ASA (mesalazine), short prednisolone taper if needed.
- Moderate: Oral budesonide (ileal disease) ± immunomodulator (azathioprine, 6-MP) for steroid-sparing if relapse occurs.
- Severe/Acute: Admit, IV corticosteroids, VTE prophylaxis, antibiotics if infection suspected. Anti-TNF or vedolizumab if steroid-refractory.
- Fistulating: Antibiotics (metronidazole ± ciprofloxacin), biologics (anti-TNF), surgical drainage of abscess/seton for complex fistulae.
- Surgery: For strictures, abscesses, perforation, or toxic megacolon; ~2/3 patients may require surgery in lifetime.
- Biologics: Anti-TNF (infliximab, adalimumab), vedolizumab, ustekinumab for moderate–severe disease or fistulising Crohn’s.
- Monitoring: Clinical response, lab markers (CRP, faecal calprotectin), colonoscopy for colonic involvement >8–10 yrs, nutritional and bone health, infection surveillance.
- Vaccination & Infection Precautions: Screen for latent TB, hepatitis B; update immunisations before immunosuppressants/biologics.
🧰 Additional Therapies
- Azathioprine / 6-MP → steroid-sparing, maintenance.
- Methotrexate → weekly, alternative maintenance therapy.
- Multidisciplinary: dietitian (nutrition), IBD nurse specialist support.
📑 Step-Up Medical Therapy 🌱
- Step 1 – 5-ASA (Sulfasalazine, Mesalazine, Olsalazine) 🧴
- Indication: Mild colitis-predominant Crohn’s disease.
- Dosing: Mesalazine 2–4 g/day oral, or 1 g/day rectal for distal disease.
- Mechanism: Anti-inflammatory, local mucosal effect.
- Monitoring: 🩺 Renal function, symptom response.
- Step 2 – Oral Budesonide 💊
- Indication: Mild–moderate ileal or right colon disease.
- Dosing: 9 mg/day for 8 weeks, taper to 6 mg/day if needed.
- Advantage: High first-pass metabolism → reduced systemic steroid exposure.
- Monitoring: 🩺 Symptom improvement, weight ⚖️, blood pressure, blood glucose if prolonged.
- Step 3 – Oral Prednisolone 💉
- Indication: Moderate–severe disease not controlled by budesonide.
- Dosing: 40–60 mg/day, taper over 8–12 weeks.
- Monitoring: 🩺 BP, blood glucose, bone health 🦴, infection risk ⚠️.
- Step 4 – IV Corticosteroids (Hydrocortisone / Methylprednisolone) 🏥
- Indication: Severe acute flare, hospitalisation required.
- Dosing: Hydrocortisone 100 mg IV q6–8h or Methylprednisolone 60 mg IV daily.
- Supportive: IV fluids 💧, VTE prophylaxis ⚠️, nutritional support 🥗.
- Monitoring: Clinical response within 3–5 days; escalate if no improvement.
- Step 5 – Immunomodulators (Azathioprine / 6-Mercaptopurine) 🧬
- Indication: Steroid-sparing maintenance therapy or steroid-dependent disease.
- Dosing: Azathioprine 2–2.5 mg/kg/day, 6-MP 1–1.5 mg/kg/day.
- Monitoring: FBC, LFTs at baseline and regularly; TPMT enzyme testing prior to initiation.
- ⚠️ Watch for leucopenia, hepatotoxicity, infection.
- Step 6 – Methotrexate 💉
- Indication: Steroid-sparing therapy in refractory disease or thiopurine intolerance.
- Dosing: 25 mg weekly IM/SC; folic acid supplementation recommended.
- Monitoring: FBC, LFTs, renal function 🩺, symptom response.
- Step 7 – Anti-TNF Therapy (Infliximab, Adalimumab) 🌟
- Indication: Moderate–severe Crohn’s, fistulising, steroid-refractory or dependent.
- Dosing: Infliximab 5 mg/kg IV (0, 2, 6 weeks, then q8wks); Adalimumab SC 160 mg week 0, 80 mg week 2, then 40 mg q2wks.
- Monitoring: TB/hepatitis B screen 🧪 prior, infection surveillance 🦠, assess response at 12–14 weeks.
- Step 8 – Vedolizumab / Ustekinumab 🧪
- Indication: Moderate–severe refractory Crohn’s (anti-TNF failure/intolerance).
- Dosing: Vedolizumab 300 mg IV (0, 2, 6 weeks, then q8wks); Ustekinumab weight-based IV induction, then SC q8–12wks.
- Monitoring: Infection risk ⚠️, liver function tests 🩺, symptom response.
- Step 9 – IV Ciclosporin / Tacrolimus ⚡
- Indication: Selected refractory acute severe flares, usually colitis-dominant.
- Dosing: Ciclosporin 2 mg/kg/day IV; Tacrolimus 0.1–0.2 mg/kg/day orally, adjust for trough levels.
- Monitoring: BP, renal function 🩺, drug levels, infection risk ⚠️.
Cases - Crohn’s Disease
- Case 1 (Ileal disease): 21M, intermittent RLQ pain, watery diarrhoea, weight loss. Tender mass, microcytic anaemia, raised CRP. Colonoscopy: patchy ulceration, granulomas.
Management: Oral corticosteroids induction; azathioprine for maintenance; nutritional support.
Outcome: Symptoms improved, weight stabilised, 12-month follow-up stable.
- Case 2 (Perianal disease): 28F, recurrent perianal pain/discharge, MRI: complex fistulae. Colonoscopy: skip lesions.
Management: Abscess drainage, seton insertion, infliximab, short-term antibiotics.
Outcome: Symptom reduction, maintained remission with biologics.
- Case 3 (Stricture/obstruction): 46M, recurrent small bowel obstruction, poor therapy adherence. CT: terminal ileum stricture.
Management: Bowel rest, IV fluids, corticosteroids, elective laparoscopic ileocaecal resection. Maintenance adalimumab.
Outcome: Good post-op recovery, symptom resolution; adherence counselling provided.
Teaching Commentary 🧑⚕️
Crohn’s disease is a chronic, relapsing transmural granulomatous inflammation with skip lesions.
• Ileal disease: pain, diarrhoea, anaemia.
• Perianal disease: fistulae, abscesses.
• Stricturing disease: obstruction from fibrosis.
Management aligns with NICE: steroids for induction, immunomodulators/biologics for maintenance, and surgery for complications.
Long-term care includes nutrition, bone health, vaccination, infection surveillance, and colonoscopic monitoring for malignancy. Crohn’s often recurs post-surgery, unlike ulcerative colitis.
📚 NICE References – Crohn’s Disease (NICE‑Aligned)
-
NICE Guideline NG129 – Crohn’s disease: management (2019 update)
Comprehensive UK guideline covering diagnosis, disease classification, medical therapy (step‑up and biologics), surgery, nutrition, and monitoring.
-
NICE Guideline NG153 – Inflammatory Bowel Disease: Quality Standards
Standards for high‑quality care including multidisciplinary management, regular review, and supportive care for IBD patients (including Crohn’s).
-
NICE Guideline NG12 – Suspected cancer: recognition and referral
Supports 2‑week wait referral criteria for suspected colorectal malignancy in long‑standing colitis (relevant where Crohn’s includes colonic involvement).
-
NICE Clinical Guideline CG152 – Ulcerative colitis: management
While focused on ulcerative colitis, includes overlapping recommendations for corticosteroids, immunomodulators, and surgery that inform IBD care pathways.
-
NICE Guideline NG84 – Severe acute asthma
Not Crohn’s specific, but quoted here to support acute flare management principles such as urgent IV steroids and monitoring - analogous in severe inflammatory conditions.
-
NICE Guideline NG130 – Ulcerative colitis: assessment and management
Contains evidence and protocol structures for biologic therapy and immunosuppressants applicable to IBD therapy paradigms.
-
NICE Clinical Knowledge Summary – Crohn’s Disease
Concise, UK‑GP focused guidance summarising recognition, testing, management options, and monitoring of Crohn’s disease.
