
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Central Retinal Arterial Occlusion (CRAO)
⚠️ Central Retinal Artery Occlusion (CRAO) is an ophthalmic emergency. 👁️ All patients should be urgently assessed by ophthalmology to exclude giant cell arteritis (GCA) and other causes. Most cases are embolic, often from carotid or cardiac sources.
ℹ️ About
- Acute occlusion of the central retinal artery → painless monocular visual loss.
- May be due to arteritis (e.g. temporal arteritis) or more commonly atherosclerosis/embolism.
- Consider CRAO as the “ocular stroke” – same vascular risk factors and prognosis.
🧬 Aetiology
- 🫀 Embolism from carotid plaque, aortic arch, or cardiac source (AF, valvular disease).
- 🔥 Vasculitis, particularly giant cell arteritis (GCA).
- Rare causes: trauma, hypercoagulable states.
Risk Factors
- 👴 Older age, ♂ male sex.
- 🚬 Smoking, hypertension, obesity, diabetes.
- 💉 Hyperlipidaemia, cardiovascular disease, arrhythmias (esp. AF).
- 🧬 Thrombophilia.
🩺 Clinical Features
- ⚡ Sudden, painless monocular visual loss (often profound).
- ⏳ May be transient (amaurosis fugax) or persistent.
- Exam: look for carotid bruit, AF, murmurs, vascular risk factors.
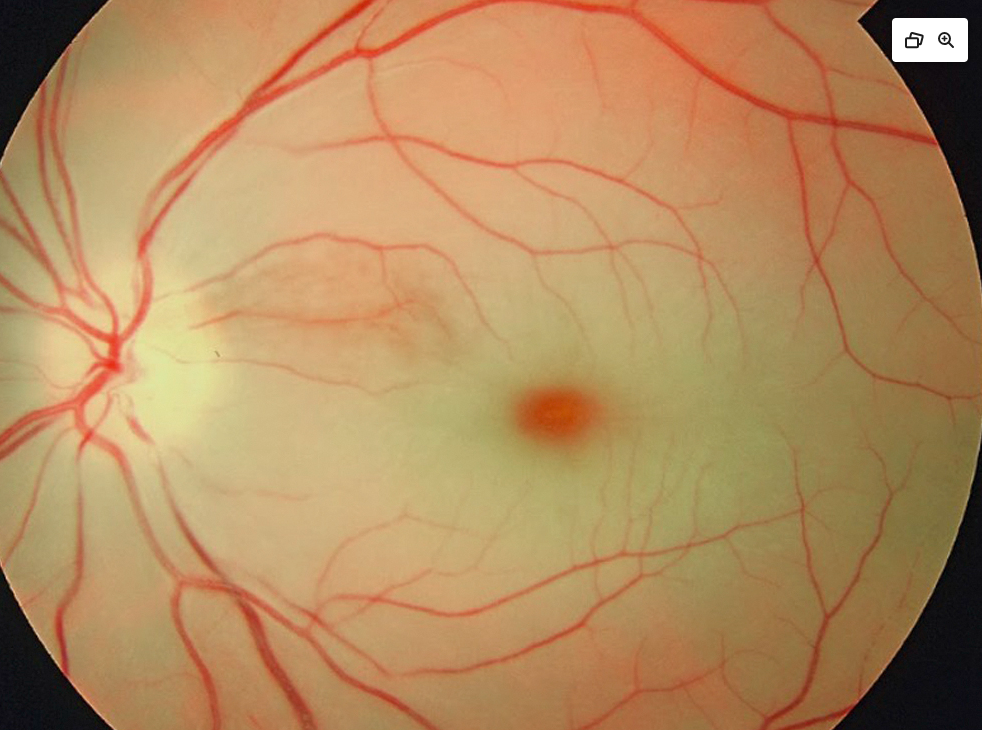
- Ophthalmoscopy: pale ischaemic retina with a cherry red spot at the macula (classic sign).
Pale Ischaemic Retina with Cherry Red Spot

Differential Diagnosis
- 🌋 Temporal arteritis (arteritic CRAO).
- 🩸 Central retinal vein occlusion (CRVO).
- 👁️ Retinal detachment.
- 🌈 Migraine aura with transient visual loss.
🔎 Investigations
- 🧪 Bloods: FBC, ESR/CRP (for GCA), U&E, glucose, lipids.
- 🫀 ECG (look for AF), echocardiogram if embolic source suspected.
- 🩻 Carotid Doppler US for stenosis/plaques.
- 🧠 MRI brain/angiography if concern for cerebral embolism or stroke.
💊 Management
- 👁️ Visual prognosis is usually poor; severity correlates with degree of retinal oedema.
- ⚡ Emergency measures (limited evidence): ocular massage, IV acetazolamide, anterior chamber paracentesis, hyperbaric oxygen. Often of questionable efficacy but may be attempted acutely.
- 💉 Consider thrombolysis if onset <4.5h, but this remains controversial and trial-dependent.
- 📉 Vascular risk reduction is key:
- Aspirin 300 mg stat then 75–300 mg OD, or Clopidogrel 300 mg stat then 75 mg OD.
- Atorvastatin 20–40 mg OD (or high-intensity statin per lipid profile).
- Anticoagulation if AF confirmed.
- 🩺 Carotid endarterectomy/stenting if ipsilateral stenosis >50% and peri-op risk is acceptable.
- 🔥 If GCA suspected: start high-dose IV/PO steroids immediately while awaiting biopsy.
References
🧾 Clinical Case 1 – Central Retinal Artery Occlusion
A 68-year-old man with a history of atrial fibrillation presents with sudden, painless loss of vision in his right eye on waking. Fundoscopy shows a pale retina with a cherry-red spot at the macula. 👉 Diagnosis: CRAO likely secondary to an embolus from atrial fibrillation. 👉 Management: urgent ocular massage, anterior chamber paracentesis, and cardiology referral for anticoagulation.
🧾 Clinical Case 2 – Central Retinal Artery Occlusion
A 55-year-old woman with longstanding hypertension and carotid artery disease presents with sudden monocular vision loss. On examination, relative afferent pupillary defect (RAPD) is present. Carotid Doppler shows severe ipsilateral carotid stenosis. 👉 Diagnosis: CRAO due to atherosclerotic embolism. 👉 Management: acute measures to restore perfusion and vascular risk factor optimisation, with urgent vascular surgery referral for endarterectomy.
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery