
| Download the amazing global Makindo app: ✅ Means NICE/National Guidelines 2026 compliant Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
Inflammatory eye disease
Related Subjects: |Episcleritis |Scleritis |Assessing a Red eye |Acute Angle Closure Glaucoma |Allergic and Infective Conjunctivitis |Anterior and Posterior Uveitis |Atropine Sulfate |Herpes simplex keratitis (HSK) |Acute Blepharitis |Chalazion
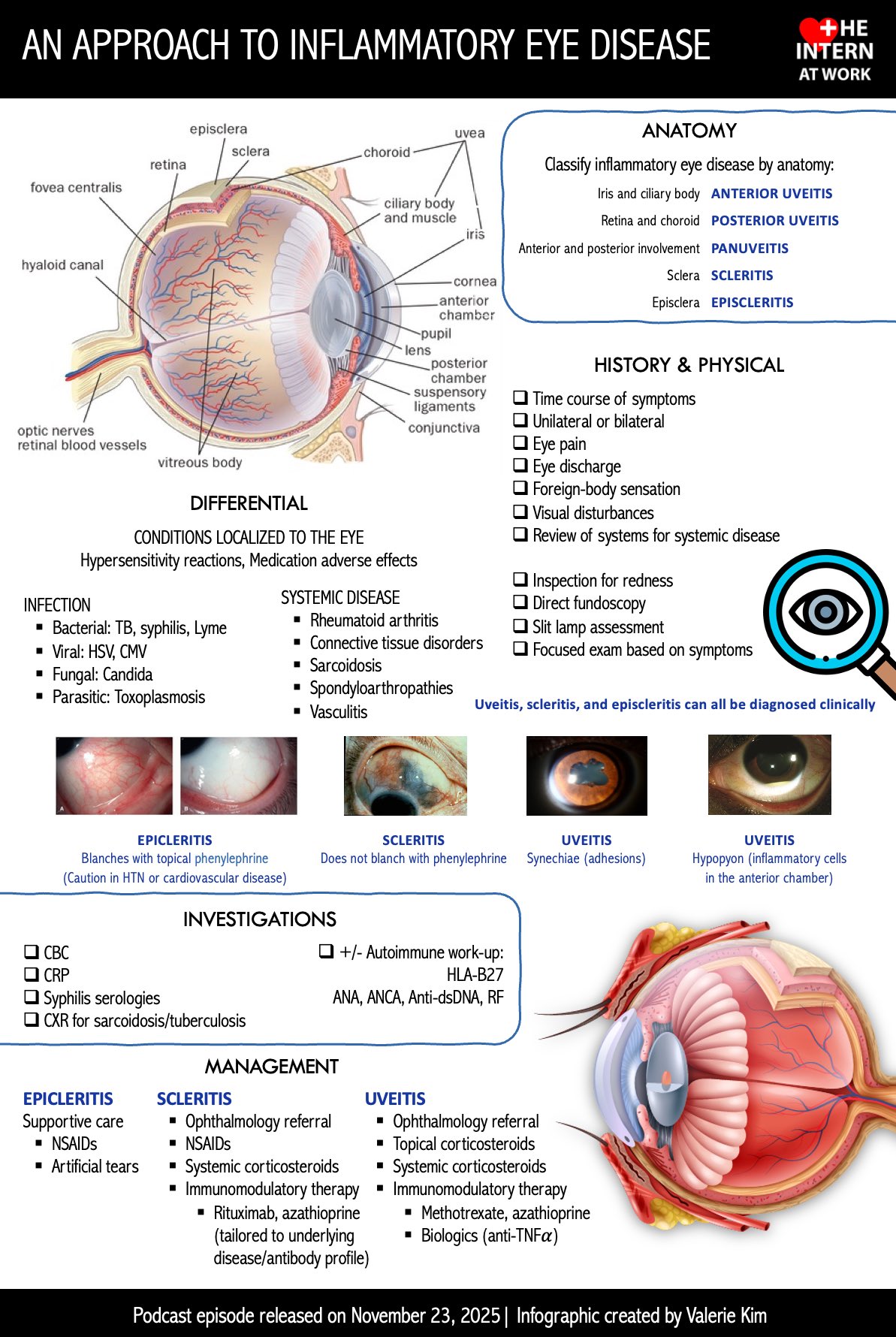
👁️ Inflammatory disease of the eye is an umbrella term for conditions where immune-driven inflammation affects the ocular surface (conjunctiva/cornea), the sclera/episclera, the uveal tract (iris–ciliary body–choroid), the retina/optic nerve, or the orbit. The high-stakes clinical point is that several inflammatory causes of a “red eye” are sight-threatening (especially uveitis, keratitis and scleritis) and should not be treated as simple conjunctivitis. In UK pathways, NICE CKS highlights urgent referral triggers for red eye, including suspected anterior uveitis and red-flag features such as reduced visual acuity, moderate–severe pain and photophobia.
Where is the inflammation?
- Conjunctivitis (inflammatory but often allergic/irritant or infective) – gritty/itchy, discharge; vision typically normal.
- Keratitis / corneal ulcer – corneal inflammation (often microbial); pain + photophobia + reduced vision; contact lens wear is a major risk marker and lowers the threshold for urgent review.
- Episcleritis – superficial inflammation; sectoral redness, mild ache/tenderness; usually self-limiting and vision is not affected.
- Scleritis – deep scleral inflammation; classically severe “boring” pain and tenderness; may threaten vision (necrosis/complications) and is associated with systemic autoimmune disease/vasculitis.
- Uveitis – inflammation of iris/ciliary body/choroid (anterior/intermediate/posterior/panuveitis); photophobia and blurred vision are common; can cause macular oedema, cataract, glaucoma.
- Retinal vasculitis / optic neuritis – inflammatory posterior-segment or neuro-ophthalmic disease; presents with visual loss/field defects (optic neuritis often has pain on eye movement).
- Orbital inflammatory disease – painful swollen eye ± diplopia/proptosis; overlaps clinically with orbital cellulitis and needs urgent assessment.
Red flags in a “red eye” (when to escalate urgently)
NICE CKS lists red-flag symptoms/signs that suggest serious or potentially sight-threatening causes of red eye-particularly reduced visual acuity, moderate to severe pain, and photophobia. These features push you toward urgent ophthalmology assessment rather than empirical primary-care treatment.
- Reduced vision or marked drop in visual acuity.
- Photophobia (often anterior uveitis or keratitis/corneal ulcer).
- Moderate–severe pain, deep tenderness, or pain on eye movement.
- Corneal opacity/haze, corneal staining/ulcer, or contact lens wearer with pain/redness.
- Abnormal pupil (small/irregular, or abnormal reactions).
- Systemic risk: immunosuppression, autoimmune disease, recent ocular surgery, trauma/chemical exposure.
Uveitis (iritis and beyond) - anatomy & pathophysiology
The uvea (iris, ciliary body, choroid) is highly vascular and immunologically active. In uveitis, inflammation disrupts the blood–aqueous and/or blood–retinal barriers, allowing protein leak (“flare”) and inflammatory cells (“cells”) into ocular chambers; posterior involvement can inflame retina/choroid and drive macular oedema, a major cause of visual loss. Clinically, anterior uveitis tends to cause photophobia, ciliary flush, ache, small/irregular pupil and blurred vision, whereas posterior uveitis may be more painless but causes floaters/visual loss. NHS and tertiary eye centres emphasise urgent assessment when pain, light sensitivity, marked redness, or vision change occurs.
- Anterior uveitis: pain, ciliary flush, photophobia, blurred vision; keratic precipitates; posterior synechiae can distort the pupil.
- Intermediate uveitis: floaters, blurred vision; vitreous inflammation (vitritis).
- Posterior uveitis: decreased vision, floaters; often less painful; can scar retina/choroid.
- Panuveitis: inflammation of anterior + posterior segments.
NICE / UK referral guidance for suspected uveitis
NICE CKS (Uveitis) advises that people with uveitis should be managed by an ophthalmologist and that an urgent (same-day) ophthalmology referral should be arranged for suspected uveitis (new or recurrent), particularly if there is a significant reduction in vision. NICE CKS (Red eye) also flags suspected anterior uveitis for urgent (within 24 hours) referral when assessing red eye presentations.
- Urgent same-day ophthalmology referral: suspected uveitis (especially if vision reduced).
- Urgent within 24 hours: suspected anterior uveitis in the red eye pathway.
5) Episcleritis vs scleritis (common diagnostic trap)
- Episcleritis (usually benign)
- Symptoms: sectoral redness, mild ache/tenderness; vision typically unaffected.
- Course: often self-limiting; lubricants and simple analgesia may suffice; referral depends on recurrence/severity/diagnostic doubt.
- Scleritis (potentially sight-threatening)
- Symptoms: severe deep pain (often worse at night), tenderness, pain with eye movement; may reduce vision.
- Why it matters: can be associated with systemic autoimmune disease/vasculitis and can lead to tissue necrosis and visual impairment if untreated.
- Referral urgency: included in emergency/urgent referral tables used in optometry pathways.
6) Keratitis (corneal inflammation) - treat as sight-threatening until proven otherwise
The cornea is avascular and depends on a healthy epithelium and tear film for defence. When the epithelium breaks (trauma, contact lenses, dry eye) microbes or immune inflammation can invade the stroma, leading to scarring and permanent visual loss; pain and photophobia are often prominent because the cornea is densely innervated. In a painful red eye with photophobia or reduced vision-especially in a contact lens wearer-urgent slit-lamp assessment is the safe default.
- Clues: pain, photophobia, foreign body sensation, blurred vision, corneal opacity or fluorescein staining.
- High-risk: contact lens wear, immunosuppression, recent corneal trauma, previous herpetic disease.
- Action: urgent ophthalmology for corneal examination, staining, and targeted treatment.
7) Systemic inflammatory associations (think beyond the eye)
- HLA-B27 spondyloarthropathies: recurrent acute anterior uveitis.
- Sarcoidosis: granulomatous uveitis, lacrimal gland involvement.
- Behçet disease: explosive relapsing uveitis/retinal vasculitis.
- Rheumatoid arthritis / vasculitis: scleritis, peripheral ulcerative keratitis.
- IBD: episcleritis and uveitis can track systemic activity.
- Infections that mimic inflammatory disease: HSV/VZV, TB, syphilis (important because steroid treatment can worsen uncontrolled infection).
8) Practical assessment (GP/AMU/ED style)
- History: onset (hours vs days), pain severity, photophobia, visual change, discharge/itch (allergy), contact lenses, trauma/chemical, systemic autoimmune symptoms, immunosuppression.
- Examination:
- Visual acuity (each eye separately, with correction if available).
- Pupils (shape/reactivity), pattern of redness (diffuse vs ciliary flush), corneal clarity/opacity.
- Ocular movements (pain on movement suggests deeper/orbital disease or optic neuritis).
- Medication safety rule: avoid starting topical steroids unless directed by ophthalmology (can worsen herpetic keratitis and mask infection).
9) Patient-facing UK safety-net (what to tell people)
The NHS advises urgent assessment (urgent GP or NHS 111) if a person has eye pain, sensitivity to light, changes in vision (flashing/blurring), or very red eyes, and emergency care if there is loss of vision. This is a helpful safety-net script for primary care and urgent care settings.
Summary
Inflammatory eye disease ranges from benign episcleritis to sight-threatening uveitis, keratitis and scleritis. The key discriminator is pain, photophobia, and reduced vision-features that shift you into urgent referral pathways rather than routine treatment. NICE CKS supports urgent referral for suspected anterior uveitis in red-eye presentations and urgent same-day ophthalmology referral for suspected uveitis more broadly, especially where vision is reduced.
References (UK guidance and reputable sources)
- NICE CKS: Red eye - Management of red eye (urgent referral; suspected anterior uveitis).
- NICE CKS: Red eye - Diagnosis (red flags: reduced visual acuity, moderate–severe pain, photophobia).
- NICE CKS: Uveitis - Topic/Management (urgent same-day referral for suspected uveitis).
- NHS: Uveitis (urgent symptoms and emergency advice).
- College of Optometrists: Episcleritis (self-limiting, vision usually unaffected; referral guidance).
- College of Optometrists: Scleritis (rare, severe; may lead to sight impairment).
- College of Optometrists: Annex 4 urgency of referrals table (includes scleritis, infective keratitis, iritis/uveitis).{index=20}
- Moorfields Eye Hospital: Uveitis (advises urgent attention if symptoms with pronounced blurred vision).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery