
| Download the amazing global Makindo app: Android | Apple | |
|---|---|
| MEDICAL DISCLAIMER: Educational use only. Not for diagnosis or management. See below for full disclaimer. |
ECG - Normal ECG basics ❤️
Related Subjects: |ECG Basics |ECG Axis |ECG Analysis |ECG LAD |ECG RAD |ECG Low voltage |ECG Pathological Q waves |ECG ST/T wave changes |ECG LBBB |ECG RBBB |ECG short PR |ECG Heart Block |ECG Asystole and P wave asystole |ECG QRS complex |ECG ST segment |ECG: QT interval |ECG: LVH |ECG RVH |ECG: Bundle branch blocks |ECG Dominant R wave in V1 |ECG Acute Coronary Syndrome |ECG Crib sheets |ECG - LVH |ECG - STEMI |ECG Analysis
🫀 Introduction to ECGs
Why ECGs matter: ECGs translate cardiac electricity into patterns you can learn. Start every trace the same way:
calibration → rate → rhythm → axis → intervals → waveforms/segments → compare with old.
✅ Normal ECGs
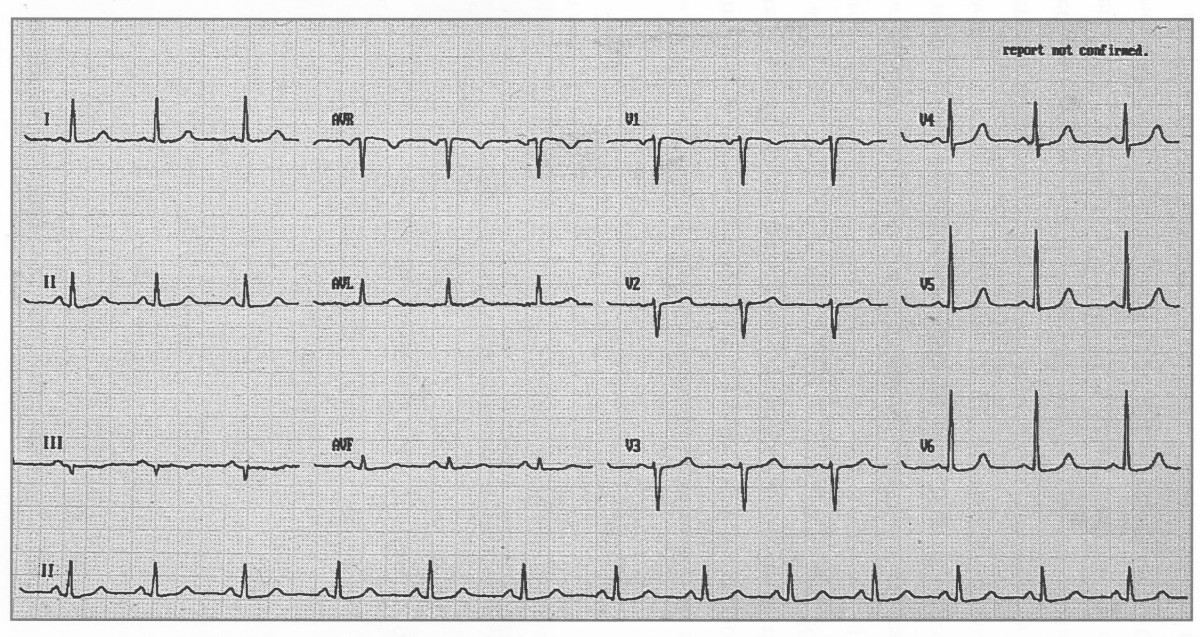
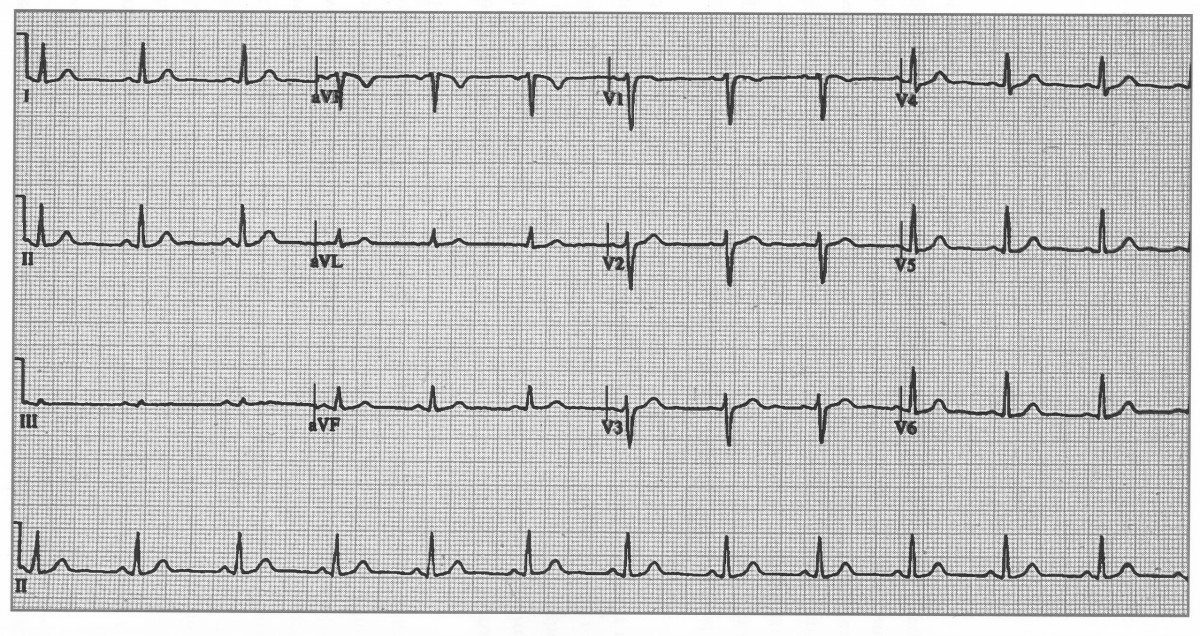
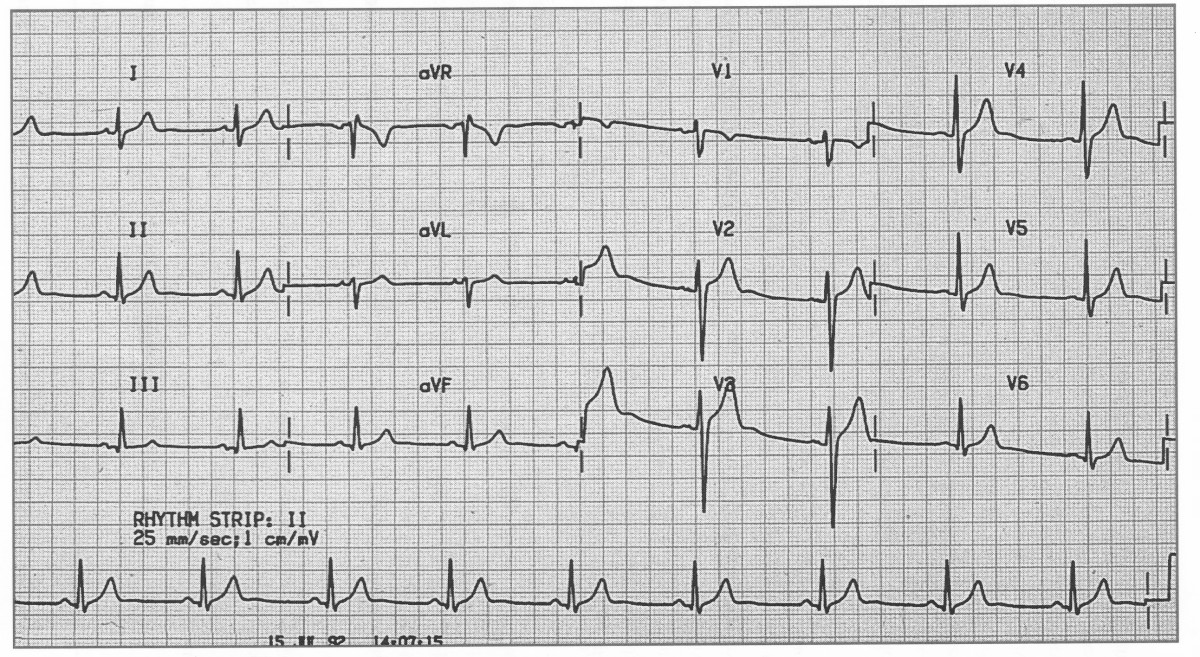
Annotated normal ECG. Sinus rhythm 60–100 bpm (this one ≈82), normal PR/QRS/QT, isoelectric ST.
🧭 The 7-Step ECG Reading Method (teach & test)
- Calibration & quality 📏 - Confirm 25 mm/s and 10 mm/mV; check artefact and lead placement (V1–V6 positions).
- Rate ⏱️ - Regular rhythm: 300-150-100-75-60-50 (big-box method). Irregular: count complexes in 10 s strip ×6.
- Rhythm 🔄 - P before every QRS? Constant PR? Narrow vs wide QRS? Sinus = upright P in I/II/aVF, negative in aVR.
- Axis 🧭 - Normal ≈ −30° to +90°. Quick check: Lead I & aVF both positive → normal; I positive / aVF negative → left axis; I negative / aVF positive → right axis.
- Intervals 📐 - PR 120–200 ms; QRS ≤120 ms; QTc <440 ms (men), <460 ms (women). Use Bazett (QT/√RR) or Fridericia (QT/∛RR) if brady/tachy.
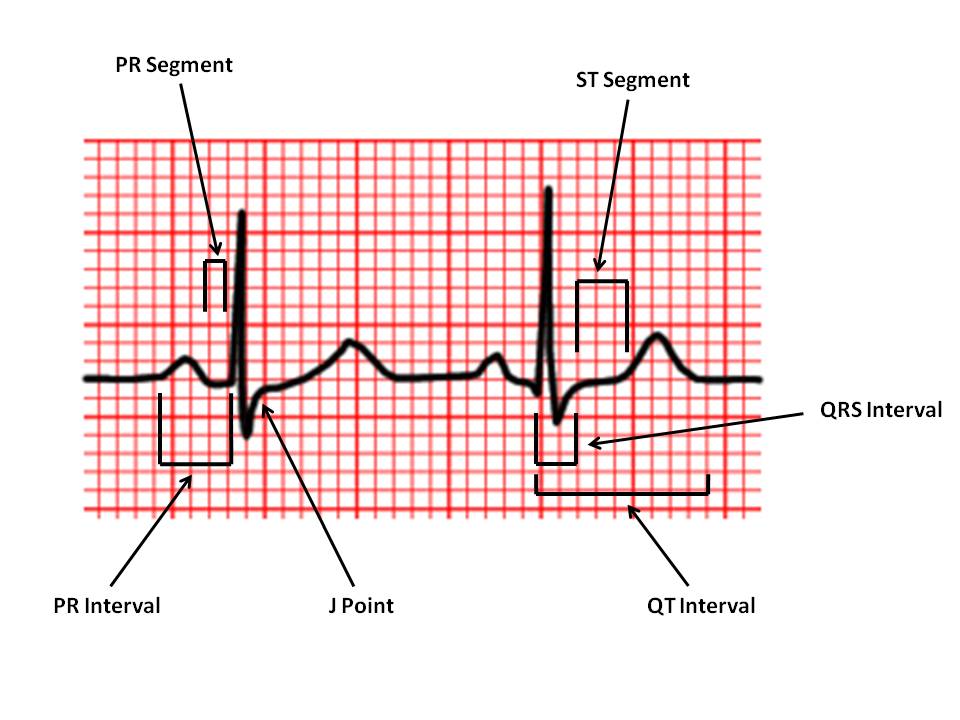
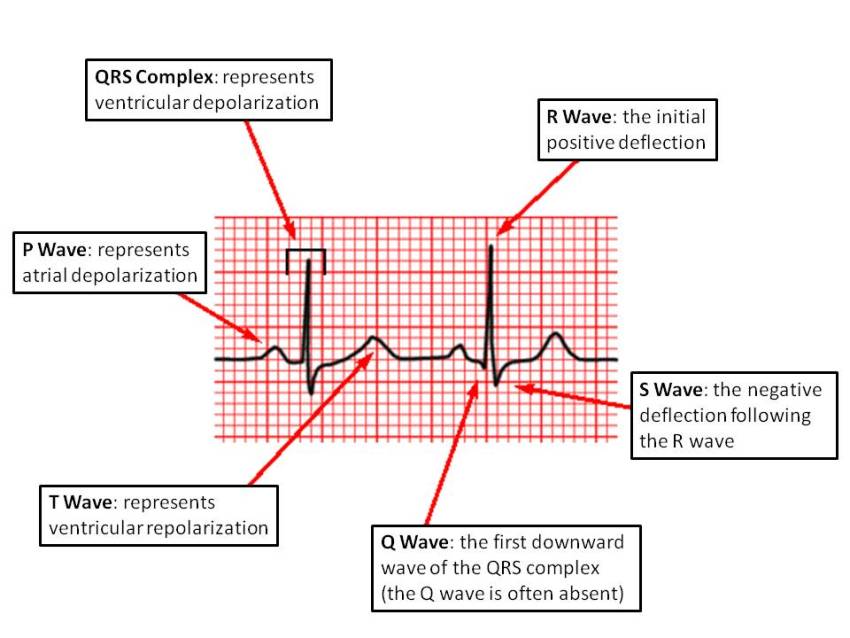
- Waves/segments 🌊 - P (morphology, P pulmonale/mitrale), QRS (hypertrophy, bundle blocks), ST (↑/↓), T (inversions, hyperacute), U waves (hypokalaemia).
- Compare 🗂️ - With prior ECGs and clinic context (pain, K+, troponin, meds like digoxin). UK practice: document “ECG unchanged vs prior”.
📏 Normal Ranges (quick reference)
| Feature | Normal | Notes |
|---|---|---|
| P wave | ≤110 ms, ≤2.5 mm height | Upright I/II/aVF, negative aVR; V1 often biphasic. |
| PR interval | 120–200 ms | Short PR: pre-excitation; long PR: AV block 1°. |
| QRS duration | ≤120 ms | Look for RBBB/LBBB patterns, delta waves. |
| QRS voltage | ≥5 mm limb lead OR ≥10 mm precordial | High voltage ≠ always LVH; check criteria + repolarisation. |
| QTc | <440 ms (M), <460 ms (F) | Correct for rate; avoid Bazett in extremes (consider Fridericia). |
| Axis | −30° to +90° | Age and body habitus influence axis. |
🧪 Pattern recognition (must-know)
- Hyperkalaemia 🔺K⁺ - Tall, peaked T; PR prolongation; QRS widening → sine-wave. Urgent calcium gluconate.
- Hypokalaemia 🔻K⁺ - Flat T, U waves, prolonged QT → torsades risk.
- Pericarditis ♨️ - Diffuse concave ST↑ with PR↓; reciprocal PR↑ in aVR; no localised reciprocal ST↓.
- STEMI ❤️🔥 - J-point ST↑ in contiguous leads (limb ≥1 mm; V2–V3 sex/age cut-offs). Look for reciprocal ST↓. New LBBB with ischaemic symptoms → treat as STEMI.
- Wellens’ ⚠️ - Deep/biphasic T in V2–V3 pain-free → critical LAD; avoid stress testing; cardiology review.
- Brugada 🧬 - Coved ST↑ V1–V3 with RBBB-like pattern → refer; fever can unmask.
- PE 🫁 - Sinus tachy, S1Q3T3, RBBB/Right axis; not sensitive-use clinical pre-test + D-dimer/CTPA.
🧠 AV & Bundle Branch Blocks (pattern drill)
| Block | ECG | Pearl |
|---|---|---|
| 1° AV | PR >200 ms, every P conducts | Often benign; watch with β-blockers, CCB, digoxin. |
| Mobitz I (Wenckebach) | PR progressively ↑ then drop | Usually AV-nodal; often transient (e.g., inferior MI). |
| Mobitz II | Fixed PR with dropped QRS | Infranodal; risk of complete heart block → pacing. |
| 3° AV (complete) | AV dissociation; escape rhythm | Unstable → atropine/chronotrope; likely pacemaker. |
| RBBB | V1 rsR′, wide S in I/V6 | May be normal variant; consider PE/ischaemia. |
| LBBB | Broad/notched R in I/V5–6, absent Q in lateral leads | Mask ischaemia; use clinical picture (Sgarbossa/Smith-mod). |
🛠️ Quick how-to: calculate rate
- Regular: 300/150/100/75/60/50 big-box method (R-R distance).
- Irregular: Count QRS in 10-second strip ×6 (or 6-second hash marks ×10).
🩺 UK exam & practice tips
- Document calibration, rate, rhythm, axis, intervals, abnormalities, and comparison: “ECG: 25 mm/s, 10 mm/mV; SR 78; normal axis; PR 160 ms; QRS 90 ms; QTc 420 ms; no ST-T changes; unchanged from 2023.”
- STEMI criteria follow UK pathways (J-point thresholds + symptoms). Don’t miss posterior MI (V7–V9) if V1–V3 ST↓ with tall R. 🚩
- Always interpret ECG in clinical context-ECG cannot “rule out” MI without symptoms/troponin. 🔬
🧩 Common pitfalls
- Misplaced chest leads → fake septal infarct (poor R-wave progression). Re-attach V1 at 4th ICS right sternal edge, V4 at 5th ICS mid-clavicular, etc.
- Calling early repolarisation “STEMI”: look for reciprocal changes, clinical pain, and evolving troponins.
- Using Bazett at extremes of rate-prefer Fridericia for tachy/brady to avoid over- or under-correcting QT.
🧪 Mini-cheat card (normal values)
PR 120–200 ms • QRS ≤120 ms • QTc <440 ms (M), <460 ms (F) • Axis −30°→+90° • R-wave progression V1→V6 with transition V3–V4 • ST isoelectric (≤1 mm variation; see sex/lead cut-offs).
| The content on this website is provided for educational and informational purposes only to support exam preparation (e.g., MLA, MRCP, USMLE) and learning. This is NOT medical advice, diagnosis, treatment, or professional guidance. It does not replace consultation with a qualified healthcare professional, official guidelines (e.g., NICE, GMC, BNF), or supervised clinical practice. Always verify information with current, authoritative sources. Makindo and its contributors accept no liability for any reliance on this content, including errors, omissions, or any resulting harm, loss, or consequences. By using this site, you agree to these terms. |
|
|
Categories
- About
- Acute Medicine
- Anaesthetics and Critical Care
- Anatomy
- Anatomy and Physiology
- Biochemistry
- Book
- Cardiology
- Collections
- CompSci
- Crib Sheets
- Critical care
- Dental
- Dermatology
- Differentials
- Drugs
- ENT
- Electrocardiogram
- Embryology
- Emergency Medicine
- Endocrinology
- Ethics
- Foundation Doctors
- GCSE
- Gastroenterology
- General Practice
- Genetics
- Geriatric Medicine
- Geriatrics
- Guidelines
- Haematology
- Hepatology
- Immunology
- Infectious Diseases
- Infographic
- Investigations
- Lists
- MRCP
- Mandatory Training
- Medical Students
- Microbiology
- Nephrology
- Neurology
- Neurosurgery
- Nutrition
- OSCE
- Obstetrics Gynaecology
- Oncology
- Ophthalmology
- Oral Medicine and Dentistry
- Orthopaedics
- Paediatrics
- Palliative
- Palliative Care
- Pathology
- Pharmacology
- Physiology
- Procedures
- Psychiatry
- Public Health
- Radiology
- Respiratory
- Resuscitation
- Revision Topics
- Rheumatology
- Statistics and Research
- Stroke
- Surgery
- Toxicology
- Trauma and Orthopaedics
- USMLE
- Urology
- Vascular Surgery