Cystitis and Urethritis (UTI)
For simple UTIs in women, treat with 3 days of antibiotics.
➡️ Use 7 days for men, pregnant women, or catheterised patients (and change the catheter).
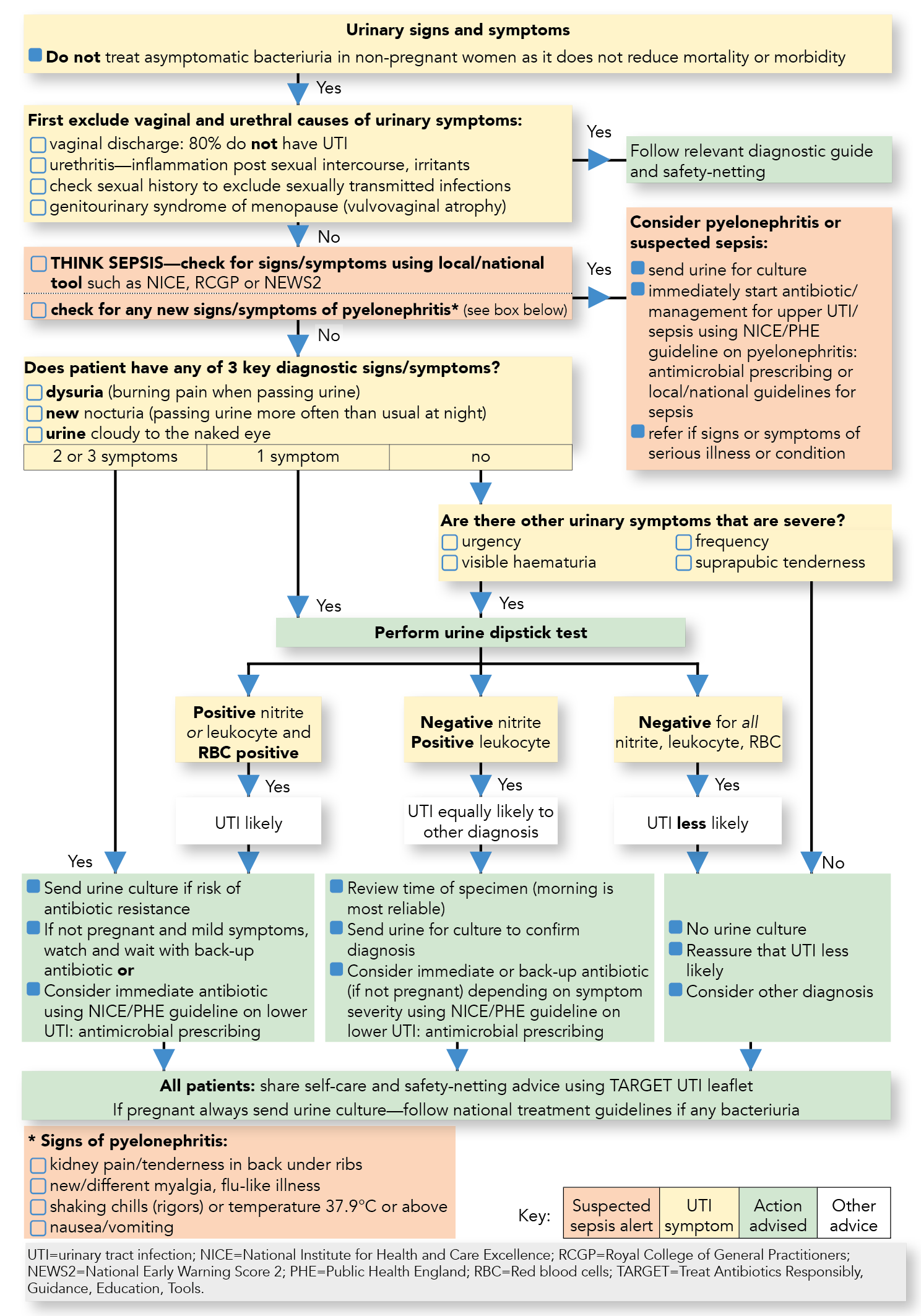
⚠️ Do NOT treat asymptomatic bacteriuria except in pregnancy or before urological procedures.
ℹ️ About
- 👩 ~30% of women experience a UTI in their lifetime.
- 👨 UTIs are uncommon in men and usually prompt further investigation.
- 🚨 Infection can ascend → pyelonephritis (flank pain, fever).
- 📡 Ultrasound: indicated in suspected upper UTI or obstruction.
📖 Definitions
- Bacteriuria: Bacteria in urine.
- Pyuria: Pus cells in urine.
- Asymptomatic Bacteriuria: >10⁵ CFU/ml, no symptoms, normal bloods.
- UTI: Bacteriuria + symptoms ± abnormal bloods.
🧾 Clinical Terms
- Frequency: Voiding >7/day (2-hourly), often with bladder inflammation.
- Urgency: Sudden need to void, often small volumes.
- Dysuria: Painful urination from urethral/bladder inflammation.
🧪 Urinalysis
- 🟢 Nitrites: Suggest Gram-negative bacteria (specific).
- ⚪ Leukocyte esterase: Indicates pyuria (sensitive, less specific).
- Both positive → send MSU for culture.
🧬 Aetiology
- Ascending infection from perineum.
- Risk factors: 💏 sexual activity, 💎 renal stones, ♿ poor bladder emptying, 🧴 catheters, 🤰 pregnancy, 💉 diabetes, 🛡️ immunosuppression.
- 👶 Children: vesicoureteric reflux → scarring risk → detect early (<5 years).
🦠 Typical Organisms
- E. coli (~70%).
- Proteus mirabilis: stone-associated.
- Klebsiella, Enterococcus faecalis.
- Staph. saprophyticus: young, sexually active women.
- Mycobacterium tuberculosis: sterile pyuria (rare).
👩⚕️ Clinical Presentation
- Foul-smelling urine, dysuria, frequency, urgency.
- Suprapubic pain, malaise, retention, ± haematuria.
- Systemic illness = suspect pyelonephritis.
🔎 Investigations
- Dipstick: Protein, leukocyte esterase, nitrites.
- Microscopy & Culture: gold standard.
💊 Management
- 🏠 Outpatient unless systemic/pyelonephritis features.
- 💧 Hydration (3+ L/day).
- Empirical antibiotics → refine after culture.
- Catheterised? Replace catheter.
- Recurrent infection → consider prophylaxis (6–12 months low-dose antibiotics).
💉 Antibiotic Choices
- Nitrofurantoin: 100 mg MR BD (avoid if eGFR <45).
- Trimethoprim: 200 mg BD (if resistance low).
- Pivmecillinam: 400 mg stat → 200 mg TDS.
- Fosfomycin: 3 g single dose.
- Amoxicillin: only if culture-proven susceptibility.
👩 Non-Pregnant Women (16+)
- First-line: Nitrofurantoin, Trimethoprim, Pivmecillinam (3 days) OR Fosfomycin (single dose).
🤰 Pregnant Women
- 7 days: Nitrofurantoin, Amoxicillin, or Cefalexin (per sensitivities).
- ⚠️ Always send urine culture.
👨 Men (16+)
- Trimethoprim or Nitrofurantoin (7 days). Avoid Nitrofurantoin if prostatitis suspected.
🛡️ Prevention
- Hydrate ≥2 L/day, void every 2–3 h.
- Void before bed & after intercourse.
- Avoid perfumed bath products.
- Prevent constipation → better bladder emptying.
📚 References
💡 Exam Pearl:
• Asymptomatic bacteriuria → treat only in pregnancy.
• Men with UTI → always investigate (rare, often structural cause).
• Dipstick alone is unreliable in >65s.
